8
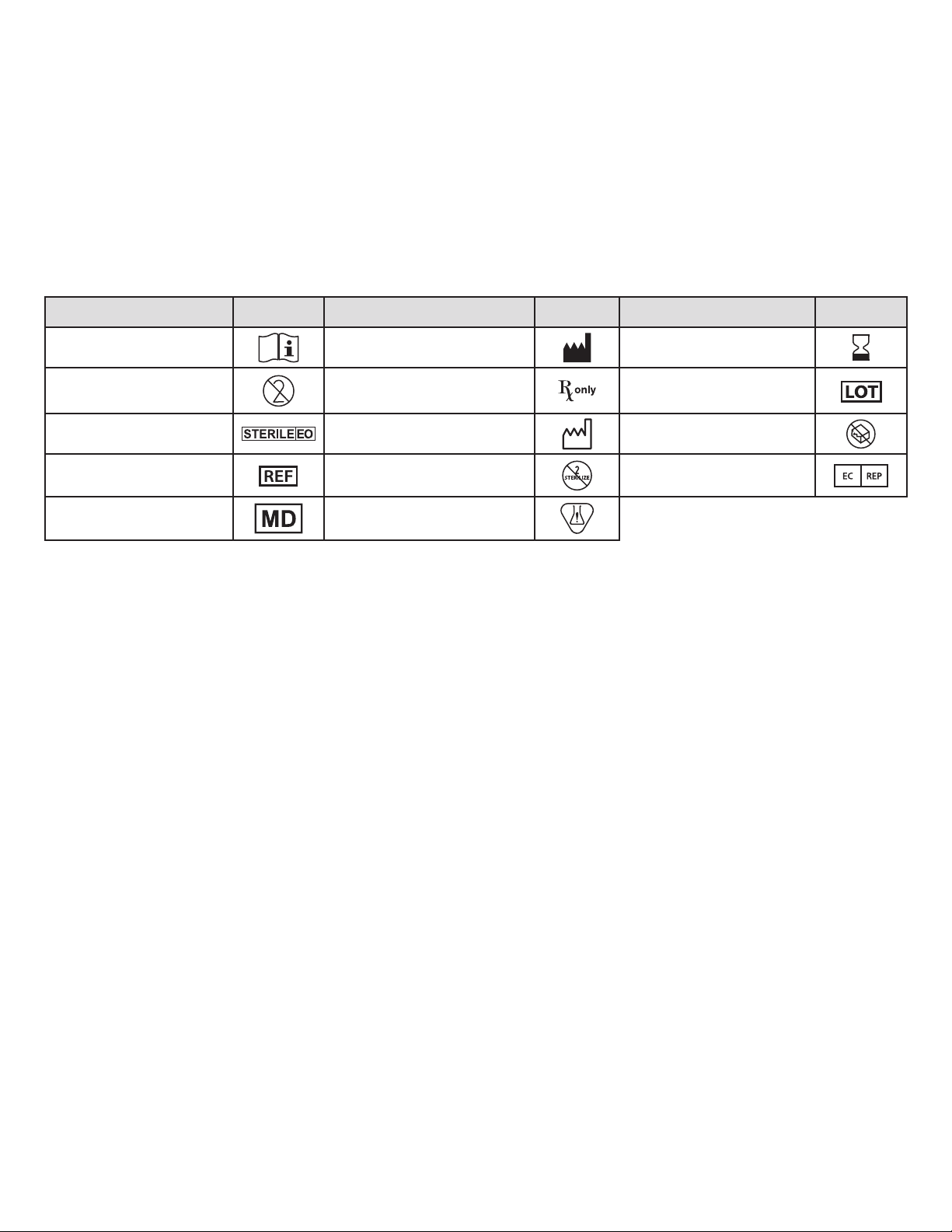
Tabla de símbolos
Para un solo uso. Desechable. No reesterilizar.
Precaución: La ley federal de EE. UU. restringe laventade este dispositivo a médicos o por prescripción facultativa.
Patente en trámite.
EXENCIÓN DE GARANTÍAY LIMITACIÓN DE RECURSOS
NO SE OTORGA NINGUNA GARANTÍA, NI EXPRESA NI IMPLÍCITA, INCLUIDAS SIN LIMITACIÓN LAS GARANTÍAS IMPLÍCITAS DE COMERCIABILIDAD O ADECUACIÓN A UN
PROPÓSITO PARTICULAR, EN LOS PRODUCTOS DE APOLLO ENDOSURGERY, INC. DESCRITOS EN ESTA PUBLICACIÓN. HASTA EL MÁXIMO GRADO PERMITIDO POR LA
LEY APLICABLE, APOLLO ENDOSURGERY INC. RECHAZA TODA RESPONSABILIDAD POR CUALQUIER DAÑO INDIRECTO, ESPECIAL, INCIDENTAL O RESULTANTE, CON
INDEPENDENCIA DE QUE DICHA RESPONSABILIDAD SE BASA EN CONTRATO, RESPONSABILIDAD EXTRACONTRACTUAL, NEGLIGENCIA, RESPONSABILIDAD ESTRICTA,
RESPONSABILIDAD POR PRODUCTOS U OTRO TIPO. LA ÚNICA Y MÁXIMA RESPONSABILIDAD DE APOLLO ENDOSURGERY, INC. POR CUALQUIER MOTIVO, Y EL ÚNICO Y
EXCLUSIVO RECURSO DEL COMPRADOR POR CUALQUIER CAUSA, SE LIMITARÁ AL IMPORTE PAGADO POR EL CLIENTE POR LOS ARTÍCULOS CONCRETOS ADQUIRIDOS.
NINGUNA PERSONA TIENE AUTORIDAD PARA VINCULAR A APOLLO ENDOSURGERY, INC. A NINGUNA DECLARACIÓN NI GARANTÍA, SALVO SEGÚN LO ESPECÍFICAMENTE
INDICADO EN LA PRESENTE. LAS DESCRIPCIONES O ESPECIFICACIONES EN EL MATERIAL IMPRESO DE APOLLO ENDOSURGERY, INC., INCLUIDA ESTA PUBLICACIÓN, TIENEN
POR OBJETO TAN SOLO DESCRIBIR EN TÉRMINOS GENERALES EL PRODUCTO EN EL MOMENTO DE LA FABRICACIÓN Y NO CONSTITUYEN NINGUNA GARANTÍA EXPRESA NI
RECOMENDACIONES DE USO DEL PRODUCTO EN CIRCUNSTANCIAS ESPECÍFICAS. APOLLO ENDOSURGERY, INC. RECHAZA EXPRESAMENTE CUALQUIER RESPONSABILIDAD,
INCLUIDA LA RESPONSABILIDAD POR DAÑOS DIRECTOS, INDIRECTOS, ESPECIALES, INCIDENTALES O RESULTANTES, DERIVADOS DE LA REUTILIZACIÓN DEL PRODUCTO.
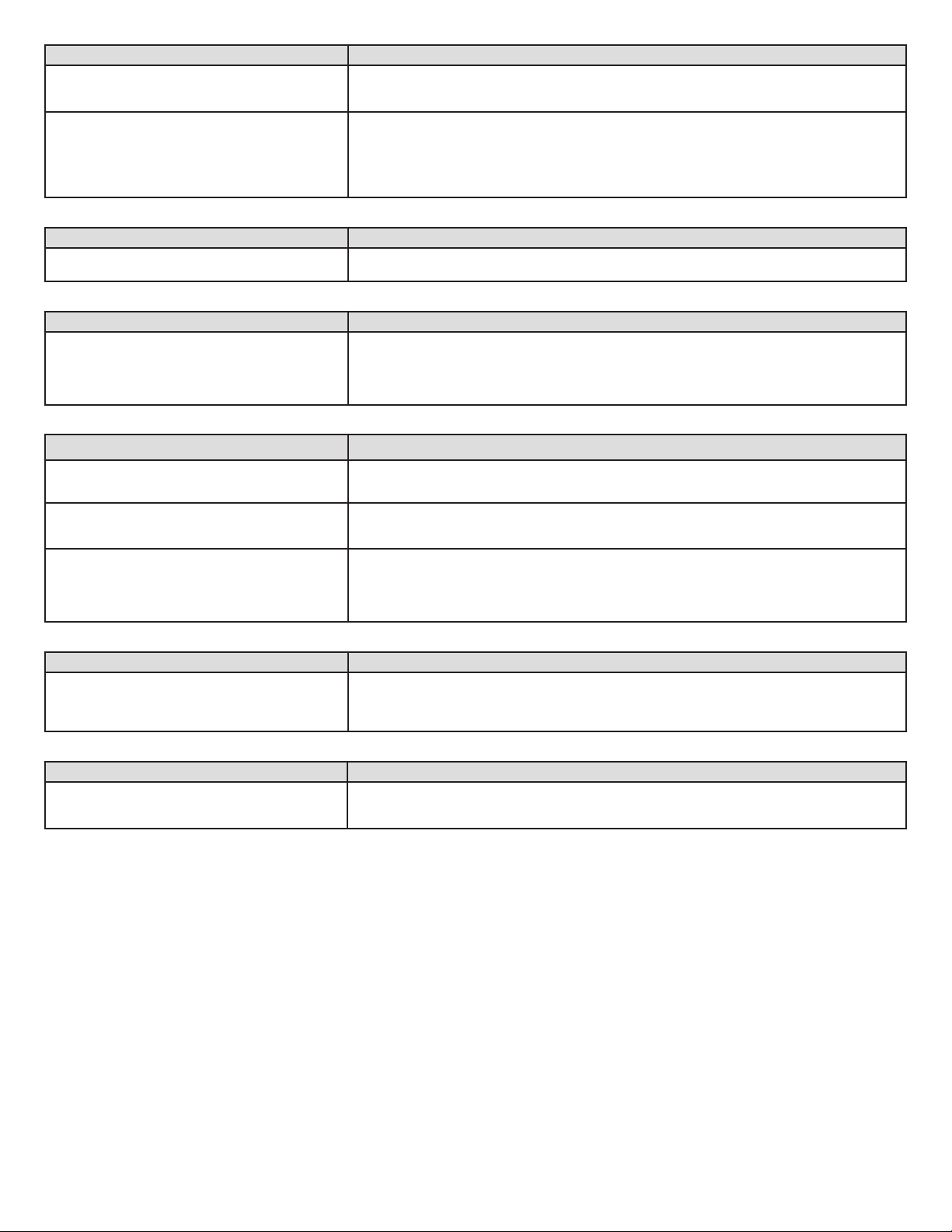
Descripción Símbolo Descripción Símbolo Descripción Símbolo
Consultar las Instrucciones de uso Fabricante Fecha de caducidad
No reutilizar
Precaución: La ley federal de EE. UU.
restringe la venta de este dispositivo
a médicos o por prescripción facultativa
Número de lote
Esterilizado con óxido de etileno Fecha de fabricación No utilizar si el envase está dañado
Número de referencia No reesterilizar Representante autorizado en la
Comunidad Europea
Producto sanitario Contiene una sustancia peligrosa
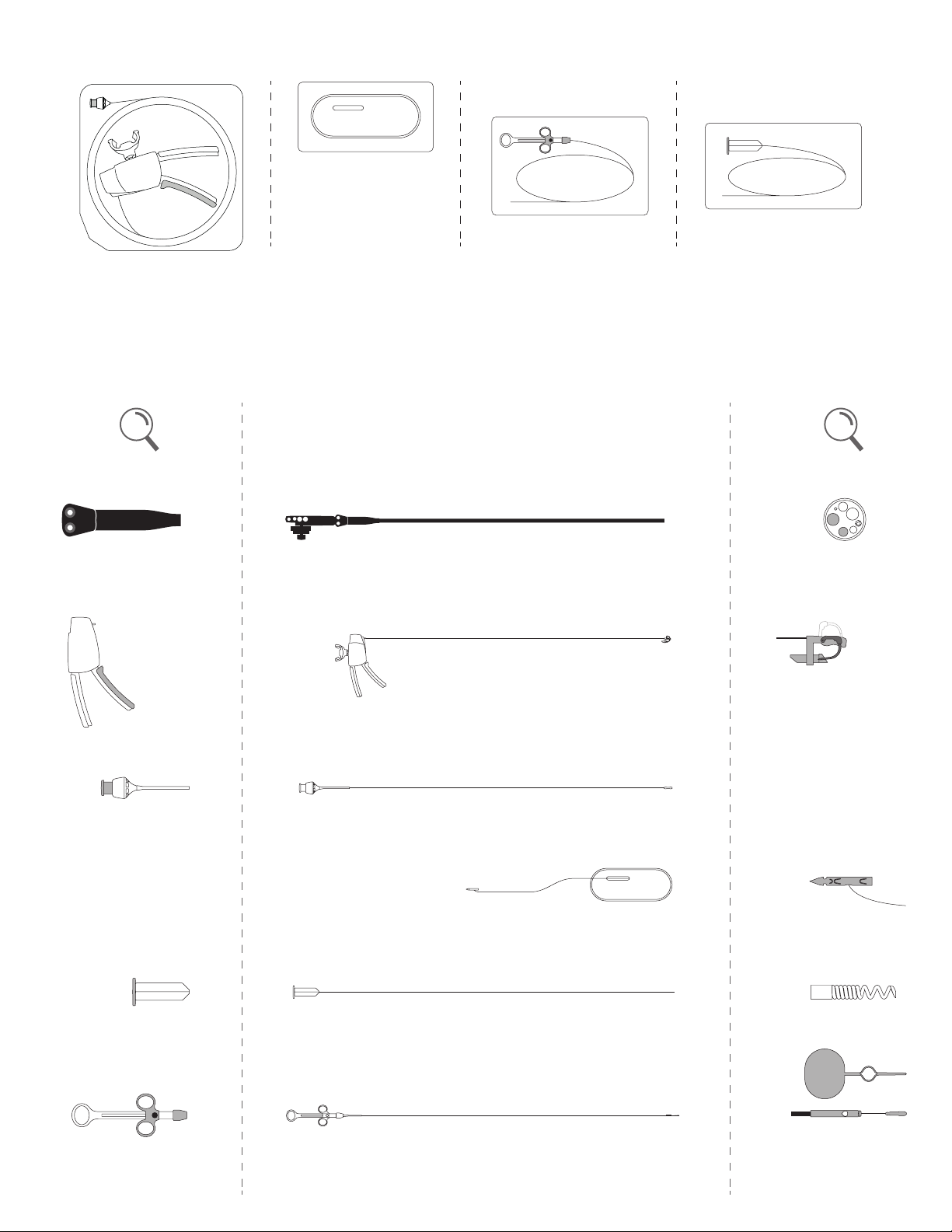
1. Uso indicado
El sistema de sutura endoscópica (SSE) OverStitch™ de Apollo Endosurgery está
indicado para la colocación endoscópica de una o más suturas y para la aproximación
de tejido blando.
1.1 Contraindicaciones
Entre las contraindicaciones se cuentan aquellas especícas del uso de un sistema de
sutura endoscópica y de cualquier tipo de procedimiento endoscópico, y pueden incluir,
entre otras, las siguientes:
• Este sistema no debe utilizarse cuando las técnicas endoscópicas
estén contrindicadas.
• Este sistema no debe utilizarse con tejido maligno.
1.2 Advertencias
• No utilice el dispositivo si la integridad del envase estéril se ha visto afectada o si el
dispositivo parece dañado.
• Solo médicos con el suciente conocimiento y experiencia en estas mismas
técnicas o en otras parecidas deberían realizar procedimientos endoscópicos.
• El contacto de los componentes electroquirúrgicos con otros componentes
puede ocasionar lesiones al paciente o al cirujano, así como daño al dispositivo
o al endoscopio.
• Verique la compatibilidad de los instrumentos y accesorios endoscópicos,
y asegúrese de que el rendimiento no se vea afectado.
NOTA: Los endoscopios reacondicionados pueden dejar de cumplir las
especificaciones originales.
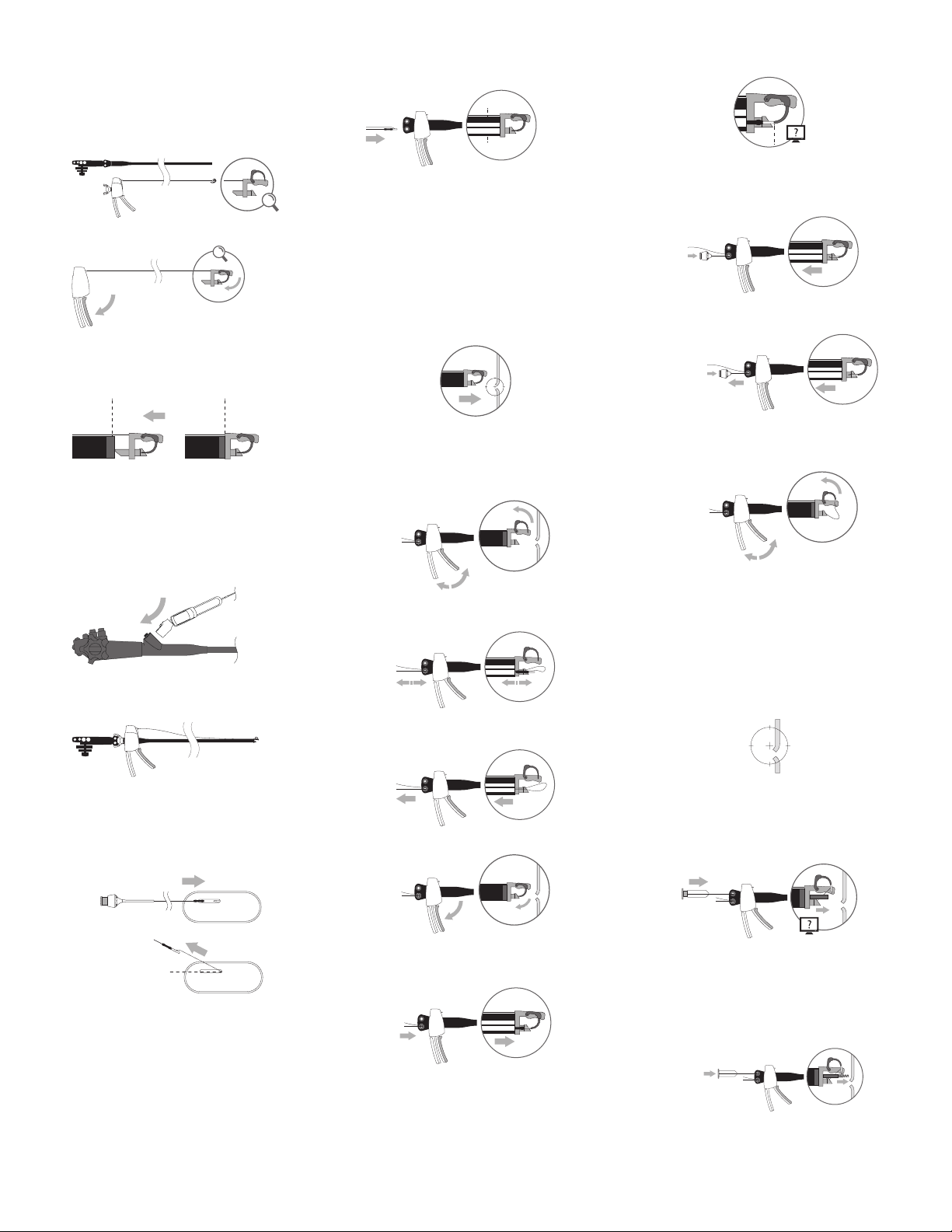
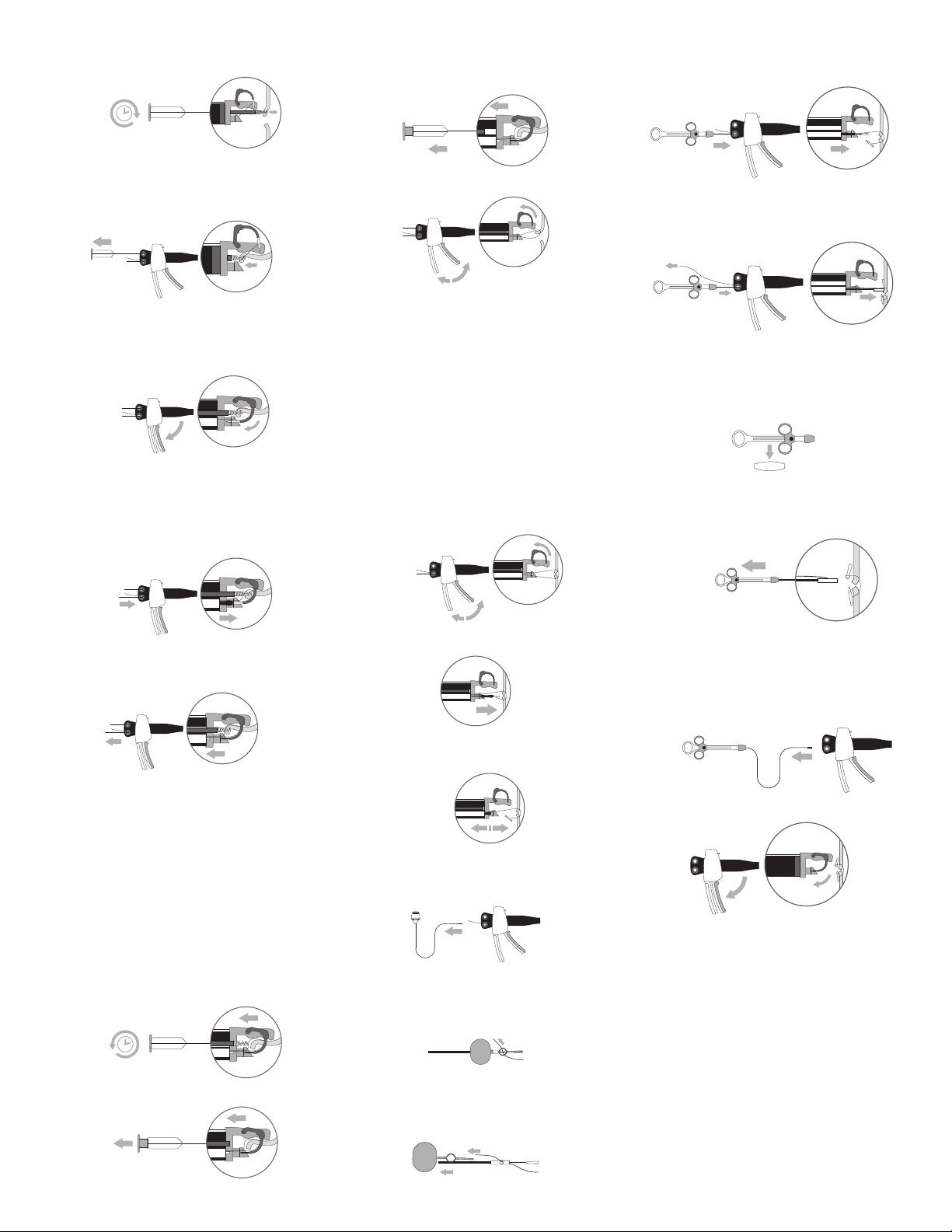
• Compruebe que haya suciente espacio para que la aguja se abra.
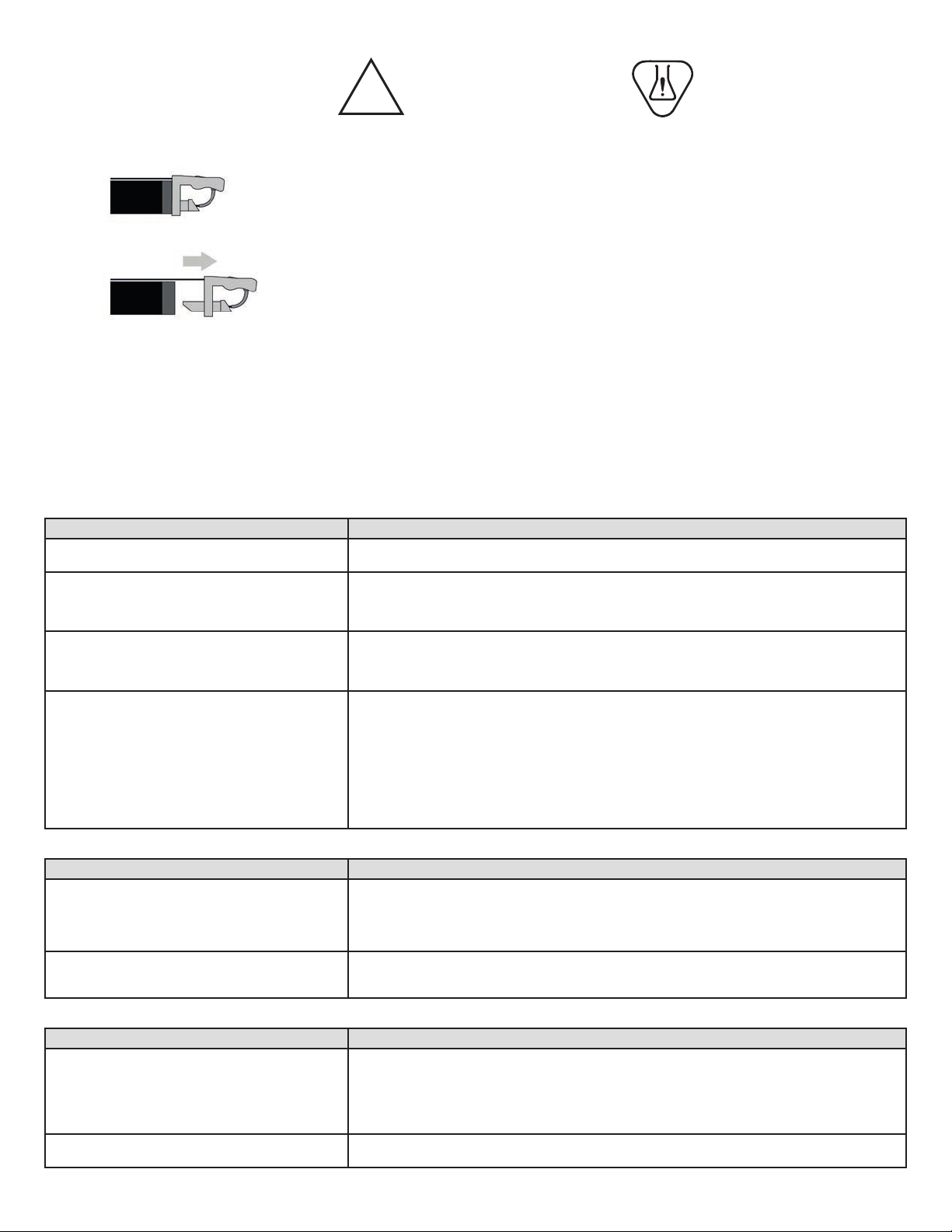
• Compruebe que el agarre del mango del sistema de sutura endoscópica esté
cerrado y bloqueado durante la intubación y la extubación.
• Los usuarios deberán estar familiarizados con los procedimientos y técnicas
quirúrgicas que utilizan suturas absorbibles antes de emplear suturas sintéticas
absorbibles para el cierre de las heridas, ya que el riesgo de dehiscencia de la
herida puede variar con el sitio de aplicación y el material de sutura usado.
• La reutilización o el reprocesamiento del sistema OverStitch podría hacer que el
sistema funcione incorrectamente o que el paciente sufra consecuencias, lo que
incluye:
–Infección o transmisión de enfermedades.
–Fallo del mecanismo del mango que haga que el dispositivo quede
bloqueado sobre el tejido y sea necesaria una intervención quirúrgica.
–Reducción de la retención sobre el endoscopio que haga que el mecanismo
de cierre terminal se desprenda durante el uso y sea necesaria una
intervención quirúrgica para recuperarlo.
–Reducción de la retención del anclaje al cuerpo de la aguja, lo que puede
provocar una caída inadvertida del anclaje que cause una demora del
procedimiento o requiera intervención posterior.
–Doblamiento del cuerpo de la aguja, lo que puede impedir que el médico
conduzca la aguja correctamente o realice el procedimiento deseado.
–Imposibilidad de extender totalmente la hélice, lo que puede limitar la
capacidad para obtener tejido y realizar el procedimiento deseado.
• Si el dispositivo mencionado se utiliza para sobresuturar cuerpos extraños, como
grapas, endoprótesis, clips o mallas, es posible que la aguja se quede atrapada en
el cuerpo extraño, lo que requeriría una intervención quirúrgica.
• En las situaciones en las que el sitio quirúrgico represente un riesgo de daños
a las estructuras anatómicas adyacentes, se recomienda el uso de accesorios
endoscópicos como la hélice para tejido OverStitch, que permite retraer el tejido
que se pretende suturar y apartarlo de estas estructuras no visibles.
1.3 Precauciones
• El sistema solo puede utilizarse si ha sido comprado directamente de Apollo
Endosurgery, Inc. o de uno de sus agentes autorizados.
• Con el sistema de sutura endoscópica instalado, el canal principal del endoscopio
se convierte de hecho en un canal de 3,2 mm.
• Se puede utilizar un tubo de inserción con un diámetro interno de al menos
16,7mm con el sistema para proteger el esófago.
1.4 Compatibilidad del sistema
El sistema de sutura endoscópica OverStitch es compatible con las suturas identificadas
en la página 1.
OverStitch es compatible con los siguientes endoscopios:
• Olympus 2T160, 2TH180 o 2T240
• Fuji EI-740D/S
La disponibilidad de dispositivos compatibles puede variar según la región.
1.5 Posibles eventos adversos
Las posibles complicaciones que pueden resultar del uso del sistema de sutura
endoscópica incluyen, entre otras:
• Faringitis/dolor de garganta
• Náuseas o vómitos
• Dolor abdominal o hinchazón
• Hemorragia
• Hematoma
• Conversión a procedimiento laparoscópico o abierto
• Estenosis
• Infección/sepsis
• Perforación faríngea, colónica o esofágica
• Laceración esofágica, colónica o faríngea
• Lesión visceral intrabdominal (hueca o sólida)
• Aspiración
• Dehiscencia de la herida
• Reacción tisular inflamatoria aguda
• Muerte
NOTA: Todo incidente grave que se haya producido en relación con el producto deberá
notificarse a Apollo Endosurgery (consulte la información de contacto al final de este
documento), así como a las autoridades oficiales pertinentes.
Español