8NGSTST |Revision: 11/15/19
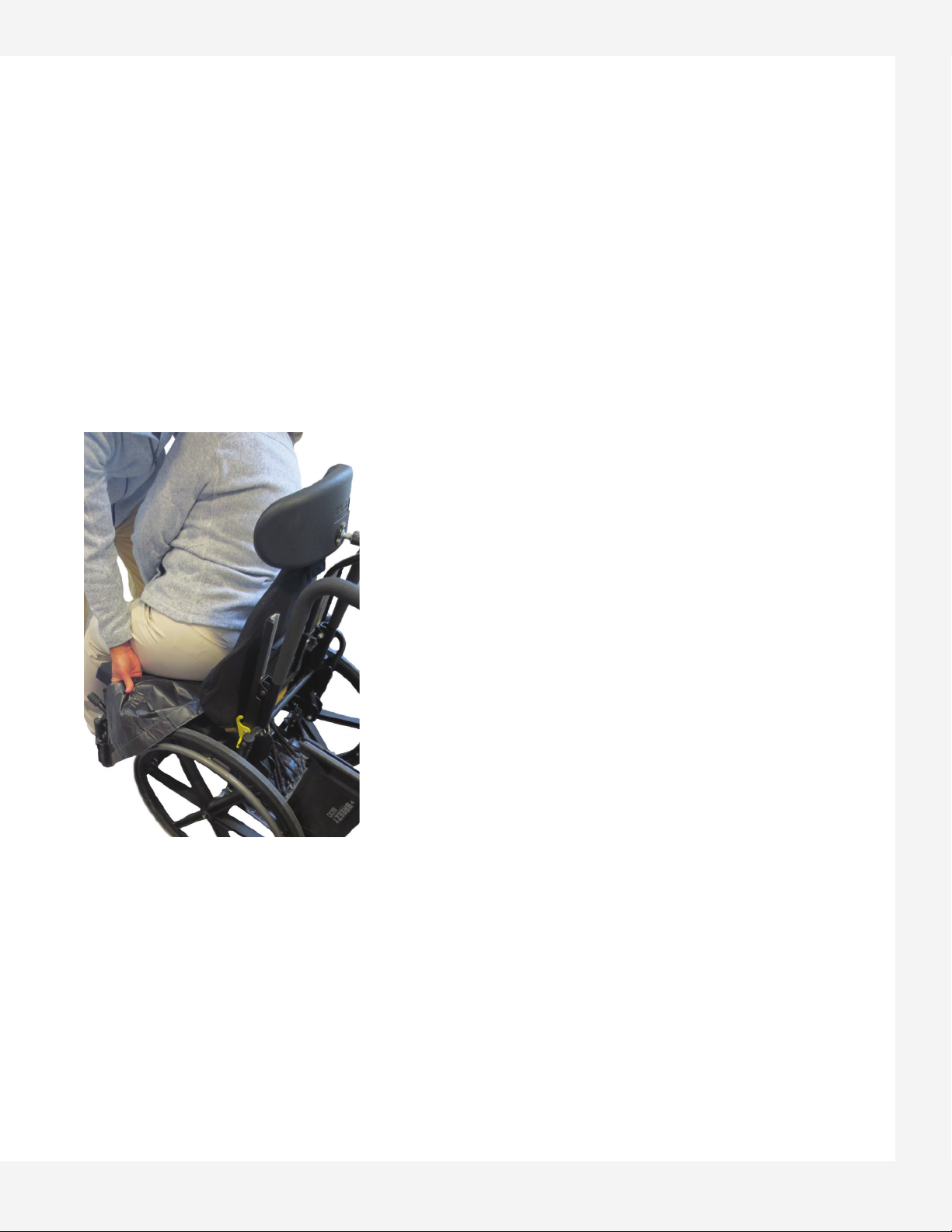
Beginning the Sit-To-Stand Practice
• Make sure that the user’s feet are flat on the floor and that
arms are extended to grasp the handlebar.
• Individuals with weak ankles may require additional support
to avoid injury at the ankle joint. This support can be provided
by the Trainer or with the use of a properly fitted splint/brace.
The ankle can be effectively trained with the NeuroGym
Ankle Trainer.
• Individuals with lower extremity flexor tone must be observed
to ensure heels do not elevate during the standing motion.
The Trainer may place a foot behind the user’s heels to ensure
feet stay flat on the ground.
• Start the training with controlled partial standing; gradually
progress to full standing.
• Observe the smoothness of the standing motion. If the user
is being pulled to standing position and contributing little
to the standing effort, reduce the counterweight. If they are
unable to achieve even a slight standing motion, increase the
counterweight. The goal is to provide the client with just
enough assistance to be able to successfully perform the
standing motion, but with as much independent effort
as possible.
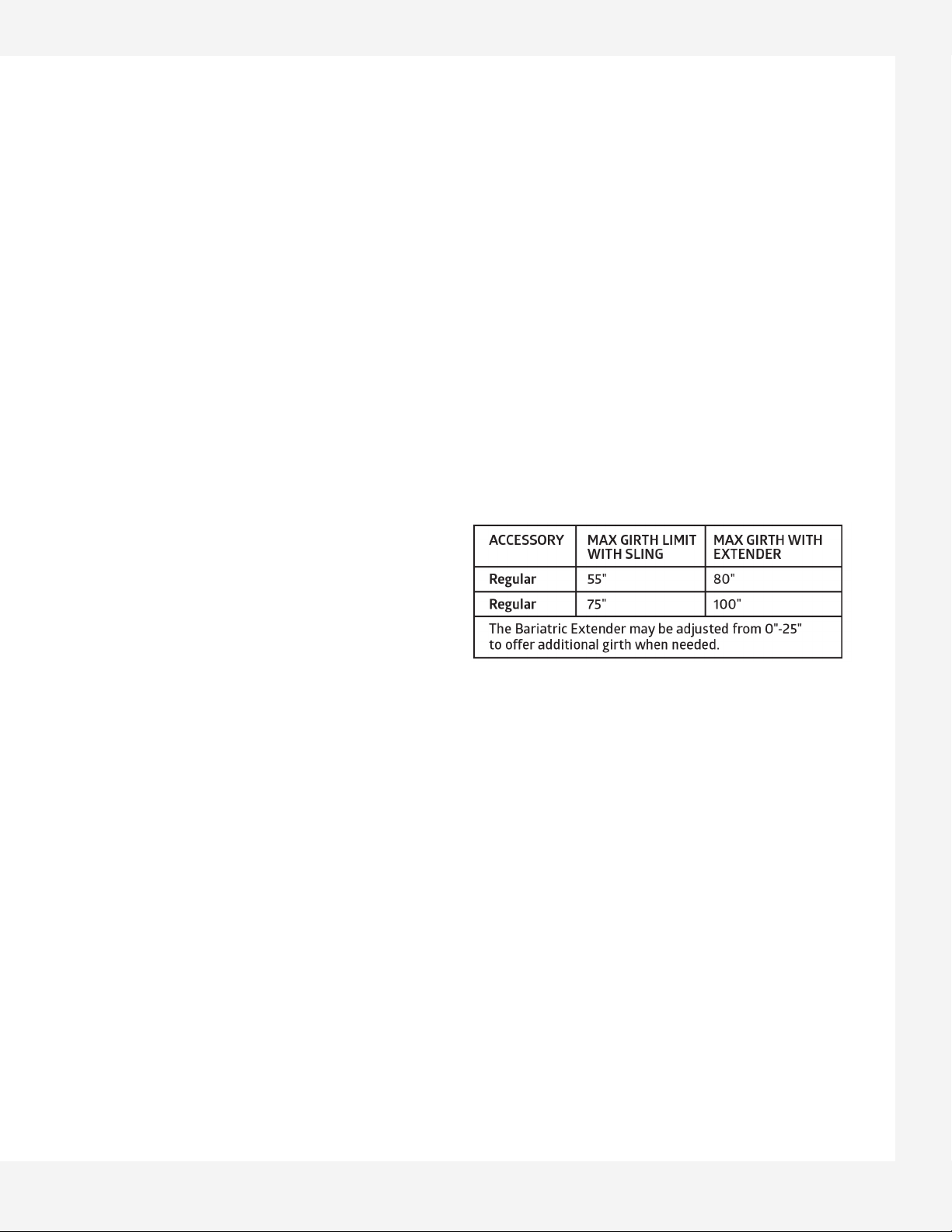
ADJUSTING THE COUNTERWEIGHT
Trainer should only adjust the counterweight when the user
is in a seated position. Disengage the weight by releasing the
Petzl while firmly gripping the rope and lower the weight down
onto the weight stack. As when pulling up a weight, make use
of body weight and lower extremities while maintaining a slight
backward lean when lowering the weight.
STANDING PRACTICE ACTIVITIES
When the correct counterweight is selected, the user may
perform repeated standing up from a seated position.
Alternatively, once standing, a squatting motion (halfway down
to a seated position and back to standing) may be practiced.
Once standing, weight shifting from one foot to the other may
also be practiced.
When standing is stable and weight shifting is performed
adequately, the trainer may unlock the wheels of the Sit-to-
Stand Trainer to allow for early first steps forward, backwards
or sideways to be taken.
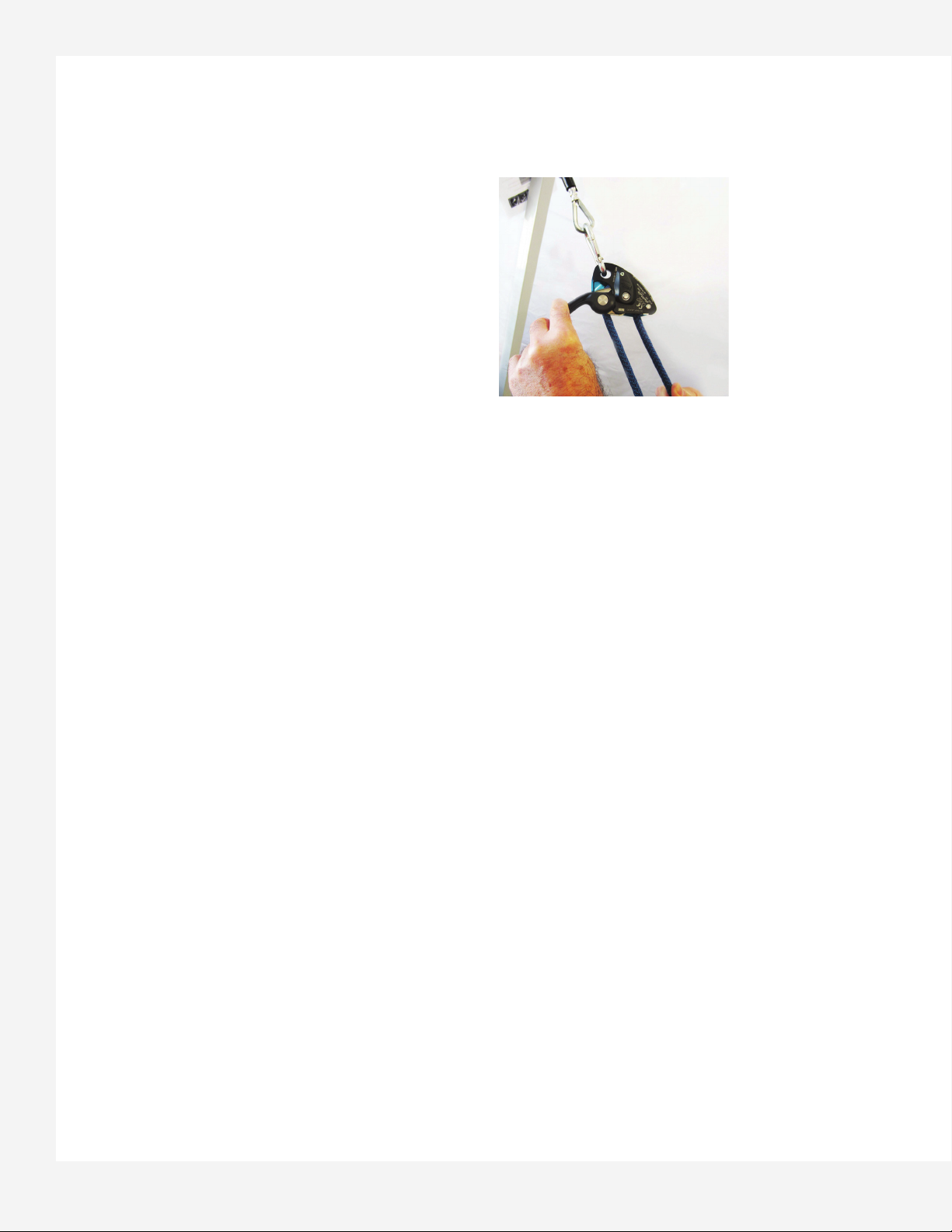
RELEASING THE PETZL
To remove a user from the Sit-to-Stand Trainer, the user should
be comfortably seated.
With one hand, slowly lift the Petzl lever, while the other hand
is placing a small amount of tension on the free end of the rope
(Figure 7). The Petzl can then be guided upwards enabling the
counterweights to be disengaged.
Once all the tension is off the rope, the sling rings can be
disconnected from the carabiner. Remove the sling from under
the user and spray inside surface with disinfectant.
Releasing the Petzl Lever:
Figure 7