Link Endo-Model 15-8007/01 User manual


Überreicht durch/Presented by:
Waldemar Link GmbH & Co. KG
Barkhausenweg 10 · 22339 Hamburg, Germany
P.O. Box 63 05 52 · 22315 Hamburg, Germany
Tel.: +49 40 53995-0 · Fax: +49 40 5386929
E-mail: [email protected] · Internet: www.linkhh.de
Wichtige Hinweise – Important Information
Please note the following regarding the use of our implants:
1. Choosing the right implant is very important.
The size and shape of the human bone determine the size
and shape of the implant and also limit the load capacity.
Implants are not designed to withstand unlimited physical
stress. Demands should not exceed normal functional loads.
2. Correct handling of the implant is very important.
Under no circumstances should the shape of a finished
implant be altered, as this shortens its life span.
Our implants must not be combined with implants from other
manufacturers.
The instruments indicated in the Surgical Technique must be
used to ensure safe implantation of the components.
3. Implants must not be reused.
Implants are supplied sterile and are intended for single use
only. Used implants must not be reused.
4. After-treatment is also very important.
The patient must be informed of the limitations of the implant.
The load capacity of an implant cannot compare with that of
healthy bone!
5. Unless otherwise indicated, implants are supplied in
sterile packaging.
Note the following conditions for storage of packaged
implants:
• Avoid extreme or sudden changes in temperature.
• Sterile implants in their original, intact protective packaging
may be stored in permanent buildings up until the “Use by”
date indicated on the packaging.
• They must not be exposed to frost, dampness or direct
sunlight, or mechanical damage.
• Implants may be stored in their original packaging for up to
5 years after the date of manufacture. The “Use by” date is
indicated on the product label.
• Do not use an implant if the packaging is damaged.
6. Traceability is important.
Please use the documentation stickers provided to ensure
traceability.
7. Further information on the material composition is available
on request from the manufacturer.
Follow the instructions for use!
Waldemar Link GmbH & Co. KG, Hamburg
All content in this catalog, including text, pictures and data, is
protected by copyright. Every instance of use, whether in part
or in whole and which is not permitted by the copyright act, is
subject to our prior consent. In particular, this applies to the
reproduction, editing, translation, publishing, saving, processing,
or passing on of content stored in databases or other electronic
media and systems, in any manner or form. The information in
the catalogs is solely intended to describe the products and does
not constitute a guarantee.
The Surgical Technique described has been written to the best
of our knowledge and belief, but it does not relieve the surgeon
of his/her responsibility to duly consider the particularities of each
individual case.
Unless otherwise indicated, all instruments are made of surgical
stainless steel.
Bei der Verwendung unserer Implantate ist Folgendes zu
beachten:
1. Die korrekte Auswahl des Implantates ist sehr wichtig.
Größe und Form des menschlichen Knochens bestimmen
Größe und Form des Implantates. Damit wird auch die
Belastbarkeit begrenzt. Implantate sind nicht dafür geeignet,
die uneingeschränkte Körperbelastung zu tragen.
Die Beanspruchung sollte nicht die normale funktionelle
Belastung überschreiten.
2. Die korrekte Handhabung des Implantates ist sehr wichtig.
Eine nachträgliche Verformung beeinträchtigt die Lebensdauer
des Implantates und darf unter keinen Umständen vorgenom-
men werden. Unsere Implantate dürfen nicht mit Implantaten
anderer Hersteller kombiniert werden.
Eine sichere Implantation der Komponenten ist nur gewährleistet,
wenn die in der OP-Anleitung benannten Instrumente verwendet
werden.
3. Kein Implantat darf wiederverwendet werden.
Die Implantate werden als sterile Einmalprodukte geliefert.
Implantate, die bereits implantiert wurden, dürfen nicht
wiederverwendet werden.
4. Die Nachbehandlung ist ebenfalls sehr wichtig.
Der Patient muss auf die Grenzen der Belastbarkeit des
Implantates hingewiesen werden. Sie ist nicht mit der
eines gesunden Knochens vergleichbar!
5. Die Implantate sind, sofern nicht anders angegeben, steril
verpackt.
Bei der Lagerung der verpackten Implantate ist Folgendes zu
beachten:
• keine starken oder schnellen Temperaturschwankungen
• Die Lagerung in der unbeschädigten Originalverpackung ist bis
zum auf dem Produktetikett angegebenen Verfallsdatum möglich
• Implantate in einem festen Gebäude lagern
• vor Frost, Feuchtigkeit, direkter Sonneneinstrahlung und
mechanischer Beschädigung schützen
• Die Lagerzeit originalverpackter Implantate ist auf maximal
5 Jahre ab Herstellungsdatum begrenzt.
Das Verfallsdatum ist auf dem Produktetikett angegeben.
• keine Implantate mit beschädigter Verpackung verwenden
6. Die Rückverfolgbarkeit ist wichtig.
Bitte verwenden Sie hierzu die der Verpackung beigefügten
Dokumentationsaufkleber.
7. Weiterführende Informationen
zu den Materialzusammensetzungen erhalten Sie auf Anfrage
beim Hersteller.
Gebrauchsanweisung beachten!
Waldemar Link GmbH & Co. KG, Hamburg
Alle veröffentlichten Beiträge, Abbildungen und Daten in diesem
Katalog sind urheberrechtlich geschützt. Jede vom Urheber-
rechtsgesetz nicht zugelassene Nutzung bedarf unserer vorhe-
rigen Zustimmung. Dies gilt insbesondere für Vervielfältigung,
Bearbeitung, Übersetzung, öffentliche Zugänglichmachung,
Einspeicherung, Verarbeitung bzw. Wiedergabe von Inhalten
in Datenbanken oder anderen elektronischen Medien und
Systemen auf jede Art und Weise und in jeder Form, ganz oder
teilweise. Die Angaben in den Katalogen dienen lediglich der
Produktbeschreibung und beinhalten keine Garantie.
Die beschriebene OP-Anleitung wurde nach bestem Wissen und
Gewissen des Herstellers verfasst. Sie kann nicht die Verantwortung
des Arztes ersetzen, den jeweiligen Besonderheiten des Einzelfalls
angemessen Rechnung zu tragen.
Alle Instrumente sind, sofern nicht anders gekennzeichnet, aus
chirurgischem Edelstahl hergestellt.

|01
Index Systembeschreibung
System Description
Indikationen/
Kontraindikationen
Indications/
Contraindications
Implantate
Implants
Instrumente
Instruments
OP-Technik
Surgical Technique
Zubehör
Accessories
Literatur
Literature
Index
Index
Sattelprothese Endo-Modell®
Endo-Model® Saddle Prosthesis
Systembeschreibung
02 Problemstellung
03 Systemübersicht
05 Indikationen/Kontraindikationen
Implantate
06 Sattelprothese
08 Prothesenschaft SPII® Modell Lubinus®
10 Instrumente
OP-Technik
12 Allgemeines
14 Spezielles: Dysplasietyp
15 Spezielles: Protrusionstyp
16 Spezielles: Resektionstyp
16 Postoperative Behandlung
17 Fallbeispiele
Zubehör
20 Sonderanfertigungen
20 Röntgenschablonen
21 Literatur
24 Index
Wichtige Hinweise
System Description
The Problem
System Overview
Indications/Contraindications
Implants
Saddle Prosthesis
Lubinus SPII® Prosthesis Stem
Instruments
Surgical Technique
General
Specifics: Dysplasia Type
Specifics: Protrusion Type
Specifics: Resection Type
Postoperative Management
Case Histories
Accessories
Custom-made Implants
X-ray Templates
Literature
Index
Important Information
Inhalt – Contents
02|
Systembeschreibung
Bei Patienten mit stark zerstörten oder resezierten
Pelvisstrukturen sind oftmals nur die oberen Anteile
des Iliums mit Resten der vorderen oder hinteren
Knochenschale erhalten. Gelegentlich fehlt sogar
die Verbindung zu den unteren Bereichen des Pelvis.
Da die oberen Anteile des Iliums bis zum Sakroiliakal-
gelenk reichen und am Gipfel der sich stark verbrei-
ternden pyramidalen Form über dem Acetabulum
eine Verdickung im kortikalen Knochen vorliegt,
fließt die Oberfläche im superior-medialen Bereich
zusammen. Weiter lateral verdünnt sich der kortikale
Knochen progressiv. Deshalb kann lediglich der
pyramidenförmig verstärkte Knochenanteil über dem
Acetabulum und der dickere mediale Bereich der
Iliumschaufel als Lager zur Abstützung eines Implan-
tates Anwendung finden.
Bei der eingangs beschriebenen Situation handelt
es sich meist um eine Revisionsarthroplastik oder
Tumoroperation, bei der das Acetabulum nicht re-
konstruiert werden kann, weil ein Transplantat nicht
refixierbar ist bzw. nicht zur Verfügung steht oder
weil dem Patienten die zeitaufwendige Operation
nicht zugemutet werden kann.
In solchen Fällen ist fast immer eine umfangreiche
Operationsplanung nötig. Dazu sind die Möglich-
keiten der Computertomografie, der Kernspintomo-
grafie, des i. v. Pyelogramms und der 3-D-Modell-
anfertigung (LINK® ComForm) zu berücksichtigen.
Zur Vereinfachung dieser Problematik kann als funk-
tionell wirkungsvolle Alternative die LINK® Sattelpro-
these Endo-Modell® eingesetzt werden.
Die Sattelprothese wurde 1979 von Nieder et al.
als Endo-Modell® Mark I entwickelt. Es handelte sich
um eine einteilige Femurprothese mit einem krück-
stockförmigen Sattel. Dieses Modell wurde 1987 zur
modifizierten Sattelprothese mit Rotation als Endo-
Modell® Mark II weiterentwickelt.
In patients with extensively damaged or resected
pelvic structures, often only the superior portions of
the ilium are preserved, with remnants of the anterior
or posterior cortical bone. Occasionally, there may
even be loss of continuity with the lower parts of the
pelvis. Since the superior portions of the ilium extend
as far as the sacroiliac joint and the cortical bone
thickens at the apex of the flared pyramidal remnant
above the acetabulum, the surface merges in the
superomedial region. More laterally, the cortical bone
gets progressively thinner.
Consequently, only the thick pyramid-shaped bone
above the acetabulum and the thicker medial area
of the iliac wing can be used for implant bearing.
The situation described above generally arises in
cases of revision arthroplasty or tumour surgery
where the acetabulum can not be reconstructed,
either because a graft can not be placed or obtained
or because the patient’s condition rules out such a
time-consuming operation.
Such cases nearly always require comprehensive
surgical planning, for which computed tomography,
magnetic resonance imaging, intravenous pyelo-
graphy and 3D modelling (LINK® ComForm) all offer
insights.
The LINK® Endo-Model® Saddle Prosthesis is an
effective alternative in such cases.
The Saddle Prosthesis was developed in 1979 by
Nieder et al. known as the Endo-Model® Mark I,
it was a one-piece femoral stem with a crutch-
shaped saddle. The model underwent further deve-
lopment in 1987, resulting in a saddle prosthesis with
axial rotation known as the Endo-Model® Mark II.
Problemstellung The Problem
|03
Index
Indikationen/
Kontraindikationen
Indications/
Contraindications
Implantate
Implants
Instrumente
Instruments
OP-Technik
Surgical Technique
Zubehör
Accessories
Literatur
Literature
Index
Index
Systembeschreibung
System Description
System Description
Die LINK® Sattelprothese Endo-Modell® Mark II
besteht aus einem symmetrischen sattelförmigen
Endstück, das direkt mit einer Mulde im Os ilium
artikuliert. Dieser Sattel steht quer zur Mulde im
Knochen, das mediale Horn im Becken, das laterale
außerhalb. Die Sattelkomponente sitzt rotations-
beweglich auf dem Zapfen des jeweiligen Basis-
teils. Zwischen Basisteil und Sattelkomponente aus
Kobalt-Chrom-Legierung ist eine hütchenförmige
Polyethylen-Laufbuchse aus UHMWPE als „Low
Friction“-Gleitpartner angeordnet. Eine Schraube,
die durch den Stumpf des Sattels in eine umlaufen-
de Nut im Zapfen des Basisteils eingreift, ohne ihr
Metall zu berühren, hilft eine Luxation dieses Gelen-
kes zu verhindern (Abb. A).
The LINK® Endo-Model® Mark II Saddle Prosthesis
consists of a symmetrical, saddle-shaped endpiece
which articulates directly with a notch in the ilium.
This saddle straddles the notch in the bone, the
medial horn lying inside the pelvis and the lateral
horn outside. The rotatable saddle component is
seated on the post of the respective base compo-
nent. Located between the base component and
the saddle component is a hat-shaped UHMWPE
sleeve which allows low-friction movement between
these two chrome-cobalt components. A screw,
which passes through the butt of the saddle to
engage a circular channel running around the post
of the base component, with-out touching the post
metal, helps to prevent joint dislocation (Fig. A).
Systemübersicht System Overview
Abb./Fig. A

04|
The base component has a female taper distally,
enabling it and the saddle (instead of the customary
ball head) to be mounted on the chosen femoral stem
component. The chosen stem components must be
designed to fit the base components. Such stem
components have a 14/16 mm taper, the interface of
which has an eccentric hole that engages the pin in
the base of the female taper of the base component,
thus preventing rotation. The base component is
additionally secured to the femoral component taper
by means of at least two fixation screws which are
screwed into two of the four distal threaded holes in
the base component and into the predrilled recesses
on the taper of the femoral component.
The articulation between saddle and base component
allows all the requisite rotational movements not
permitted by the saddle joint itself. The pivoting
movements that occur in the joint between bone and
saddle as well as the rotation between the saddle
and the base component replace the movements
permitted by the “lost” ball-and-socket joint (Fig. B).
Das Basisteil hat distal eine Konusbohrung. Damit
wird es zusammen mit dem Sattel – statt des
üblichen Kugelkopfes – auf die gewählte femorale
Schaftkomponente gesteckt. Die Schaftkomponenten
müssen auf eine Kopplung mit den Basisteilen abge-
stimmt sein. Sie haben deshalb einen Konus in der
Größe 14/16 mm, der in seiner Stirnfläche eine ex-
zentrische Bohrung aufweist, in die der Stift, der sich
am Grund der Konusbohrung des Basisteils befindet,
rotationsverhindernd eingreift. Zusätzlich gesichert
wird das Basisteil auf dem Konus der Femurkompo-
nente, indem wenigstens zwei Sicherungsschrauben
durch zwei der vier distalen Gewindebohrungen am
Basisteil in jeweils einen vorher gebohrten Rezess
am Konus der Femurkomponente eingeschraubt
werden.
Das Gelenk zwischen Sattel und Basisteil ermöglicht
alle notwendigen rotatorischen Bewegungen, die das
Sattelgelenk selbst nicht erlaubt. Die Schwenkungen
im Gelenk zwischen Knochen und Sattel und die
Rotation im Gelenk zwischen Sattel und Basisteil
ersetzen die Bewegungsmöglichkeiten des verloren
gegangenen Kugelgelenkes (Abb. B).
Abb./Fig. B
Systembeschreibung
|05
Index Implantate
Implants
Instrumente
Instruments
OP-Technik
Surgical Technique
Zubehör
Accessories
Literatur
Literature
Index
Index
Indikationen/
Kontraindikationen
Indications/
Contraindications
Systembeschreibung
System Description
K K
M M
S S
R R
System Description – Indikationen/Indications
Die Basisteile sind bajonettförmig gewinkelt und
versetzen das Femur nach lateral. Dadurch wird
auch ein Einbeinstand möglich, falls noch genügend
Abduktoren vorhanden sind (Abb. C).
The base components are angled in the shape
of a bayonet and displace the femur laterad.
This arrangement also permits standing on one leg,
providing sufficient abductors are still present
(Fig. C).
Indikationen/
Kontraindikationen
Indications/
Contraindications
Hinweis: Spezifizierte Indikationen/
Kontraindikationen siehe Seite 22.
Note: For specific indications/
contraindications, see page 23.
Abb./Fig. C

06|
Implantate
Sonderanfertigung „Sattelkomponente“ siehe Seite 20.
For custom-made saddle component, see page 20.
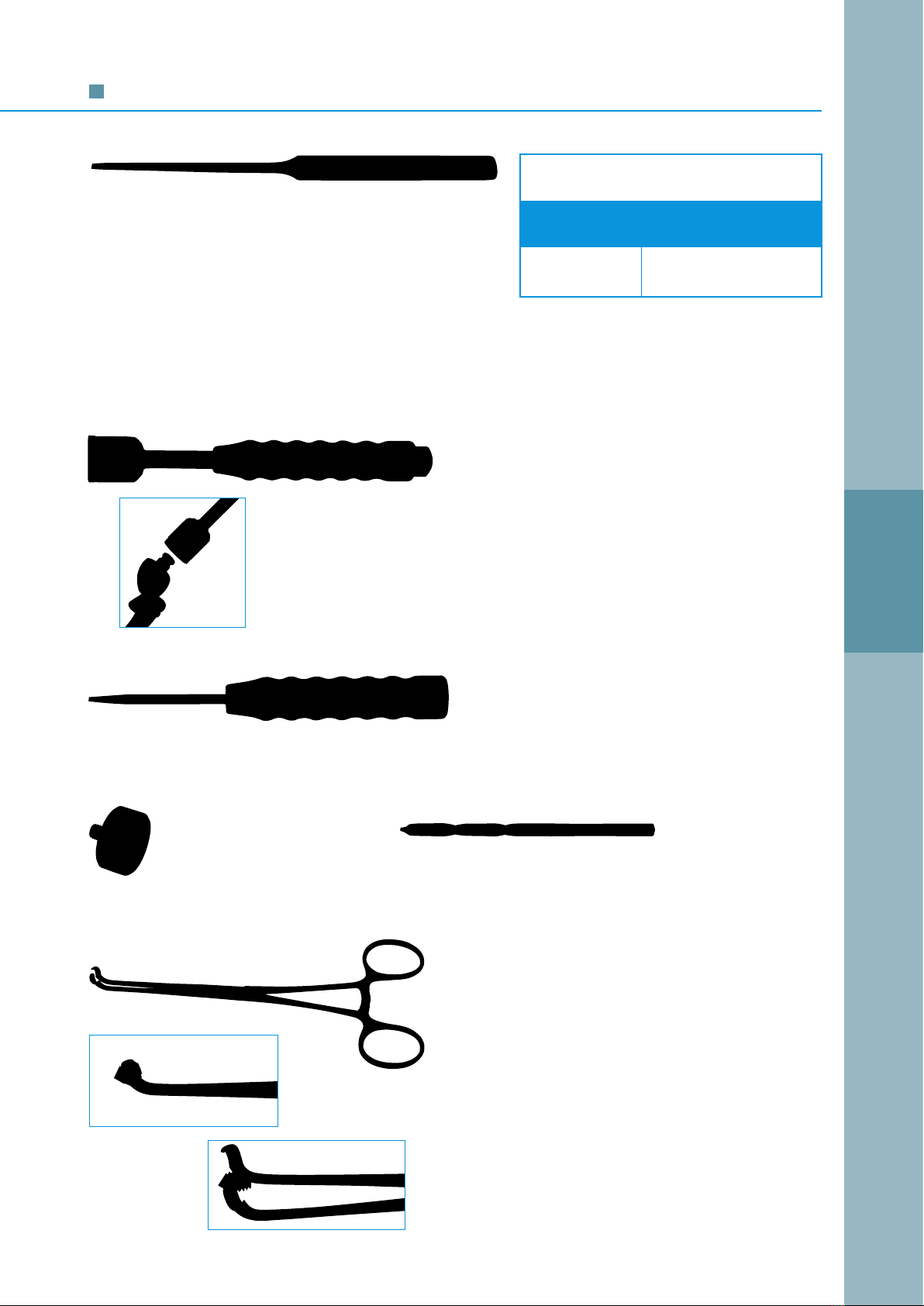
F Bohrbuchse für Spiralbohrer/Drill sleeve for twist drill
G Spiralbohrer/Twist drill
H Schraubendreher für Sicherungsschraube (Sattel) und Sicherungsmadenschraube (Basisteil)
Screwdriver for fixation screw (saddle) and set screw (base component)
Das Basisteil ist mit den beigefügten Schrauben zusätzlich am Konus zu fixieren.
Dafür stehen entsprechende Hilfsinstrumente (unten gelistet unter F bis H) zur Verfügung.
Zur sicheren Schraubenfixierung müssen unter Verwendung des Spiralbohrers und der
Bohrbuchse Sacklöcher (mind. 2, max. 4) in den Prothesenkonus eingebracht werden.
The base component must be additionally secured to the taper with the supplied set
screws. The appropriate tools are provided (F to H listed below).
To achieve a secure screw fixation, the twist drill and the drill sleeve must be used to
prepare blind holes (min. 2, max. 4) into the prosthesis taper.
Die Sattelprothese darf nur mit LINK®
Prothesenschäften mit einen Konus von
14/16 mm und stirnseitiger Bohrung zur
Aufnahme des rotationshemmenden
Zapfens am Basisteil kombiniert werden.
The Saddle Prosthesis may only be
combined with LINK® femoral stems
featuring a 14/16 mm taper and a hole
at the interface to engage the anti-
rotation pin inside the base component.
Ø/dia. 14 mm
Ø/dia. 16 mm
Sattelprothese Saddle Prosthesis

|07
Index Systembeschreibung
System Description
Indikationen/
Kontraindikationen
Indications/
Contraindications
Instrumente
Instruments
OP-Technik
Surgical Technique
Zubehör
Accessories
Literatur
Literature
Index
Index
Implantate
Implants
H
160
00
130
100
90
80
70
60
VII
VI
V
IV
III
II
I
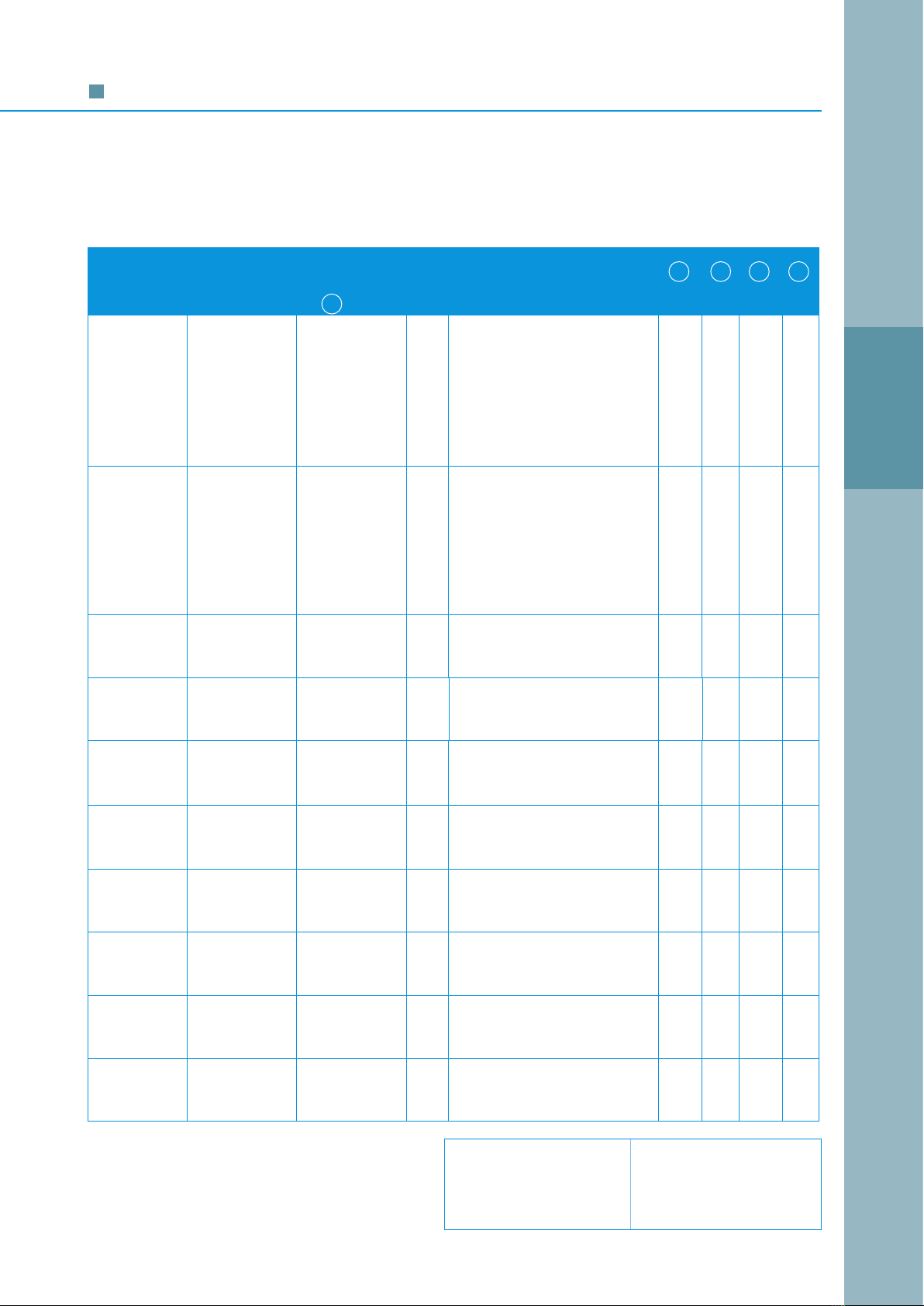
Implants
Art.-Nr.
Item No.
Größe
Size
Länge Length
(mm)
15-8007/01 I 60
15-8007/02 II 70
15-8007/03 III 80
15-8007/04 IV 90
15-8007/05 V 100
15-8007/06 VI 130
15-8007/07 VII 160
Sattelprothese, komplett, inkl. 4 Sicherungsmadenschrauben
Saddle Prosthesis, complete, incl. 4 set screws
Bestehend aus/Consisting of:
* Basisteile ohne Zapfen für Prothesenschäfte mit Konen 12/14 mm auf Anfrage.
* Base components without anti-rotation pin for femoral stems with 12/14 mm taper available on request.
** nach ISO 5832/4 /**to ISO 5832/4
*** nach ISO 5834/2 /***to ISO 5834/2
Sattel-
komponente
Saddle
component
Sicherungs-
schraube
Fixation
screw
Sicherungs-
maden-
schrauben
Set screws
Polyethylen-
Laufbuchse
Polyethylene
bearing
Basisteile mit Zapfen*
zur Rotationssicherung, Konus 14/16 mm
inkl. 4 Sicherungsmadenschrauben
Base components*
with inside anti-rotation pin, incl. 4 set
screws, 14/16 mm taper
15-8007/21 I 60
15-8007/22 II 70
15-8007/23 III 80
15-8007/24 IV 90
15-8007/25 V 100
15-8007/36 VI 130
15-8007/37 VII 160
Basisteile inkl. 4 Sicherungsmadenschrauben =
1 Verpackungseinheit
Base components, incl. 4 screws set =
1 packaging unit
15-8007/26
Satz/Set:
15-8007/13
CoCrMo** CoCrMo** UHMWPE*** CoCrMo** CoCrMo**
CoCrMo** CoCrMo** UHMWPE*** CoCrMo** CoCrMo**
(4 St./set of 4)
15-8007/12
15-8007/1115-8007/10
Für Basissattel-
Art.-Nr. Größe länge/For base
Item No. Size component length
(mm)
B
Materialien/Materials:
DECA

08|
135° CCD
Ø/dia.
14 mm
Ø/dia.
16 mm
Die Sattelprothese kann mit SPII® Modell Lubinus®, die einen Konus von
14/16 mm und ein Fangloch aufweisen, kombiniert werden.
Kombinationsmöglich-
keiten mit anderen Prothesenschäften unseres Herstellungs
programms auf Anfrage.
The
Endo-Model® Saddle Prosthesis may be combined with
14/16 mm taper
„Lubinus SPII® Prosthesis System“ femoral stems with holes for antirotation pins
.
Information on possible combinations with other LINK® femoral stems available
on request.
Implantate
Prothesenschaft SPII®
Modell Lubinus®
Lubinus SPII® Prosthesis Stem
|09
Index Systembeschreibung
System Description
Indikationen/
Kontraindikationen
Indications/
Contraindications
Instrumente
Instruments
OP-Technik
Surgical Technique
Zubehör
Accessories
Literatur
Literature
Index
Index
Implantate
Implants
Implants
Prothesenschäfte mit Fangloch
Konus 14/16 mm für Sattelprothesen,
SPII® Modell Lubinus®
Material: CoCrMo-Legierung
Prosthesis Stems with Bore Hole
14/16 mm taper for Saddle Prostheses,
Lubinus SPII®
Material: CoCrMo alloy
R = rechts/right
L = links/left
01 = extraschlank/x-narrow
1 = schlank/narrow
2 = normal/medium
3 = stark/large
4 = extrastark/x-large
45 = extrastark plus/
x-large plus
5 = superstark/super-large
The size of the femoral stem, composed of a letter and
a number, is indicated on the top of the collar:
Die Prothesenschäfte tragen auf der Oberseite
der Halsauflage eine Kennzeichnung aus je einem
Buchstaben und einer Ziffer:
Art.-Nr.
Item No.
135° CCD
Ausführung
Version
Schaftlänge
Stem length
C (mm)
Schaftstärke
Stem size
B D E G
(mm)
128-950/35 rechts right 170 R01 extraschlank x-narrow 23.5 11 7 5
128-952/35 rechts right 170 R1 schlank narrow 25.5 13 8 5
128-954/35 rechts right 170 R2 normal medium 27.5 14 9 6
128-956/35 rechts right 170 R3 stark large 29.5 15 10 6.5
128-958/35 rechts right 170 R4 extrastark x-large 31.5 16 11 7.5
128-960/35 rechts right 170 R4A extrastark plus x-large plus 31.5 18 11.5 8.5
128-962/35 rechts right 170 R5 superstark super-large 31.5 22 12.5 10
128-951/35 links left 170 L01 extraschlank x-narrow 23.5 11 7 5
128-953/35 links left 170 L1 schlank narrow 25.5 13 8 5
128-955/35 links left 170 L2 normal medium 27.5 14 9 6
128-957/35 links left 170 L3 stark large 29.5 15 10 6.5
128-959/35 links left 170 L4 extrastark x-large 31.5 16 11 7.5
128-961/35 links left 170 L4A extrastark plus x-large plus 31.5 18 11.5 8.5
128-963/35 links left 170 L5 superstark super-large 31.5 22 12.5 10
128-970/35 rechts right 200 R2 normal medium 27.5 14 11 8
128-972/35 rechts right 200 R3 stark large 29.5 15 12 9
128-974/35 rechts right 200 R4 extrastark x-large 31.5 16 13 10
128-971/35 links left 200 L2 normal medium 27.5 14 11 8
128-973/35 links left 200 L3 stark large 29.5 15 12 9
128-975/35 links left 200 L4 extrastark x-large 31.5 16 13 10
128-976/35 rechts right 250 R2 normal medium 27.5 14 11 8
128-978/35 rechts right 250 R3 stark large 29.5 15 12 9
128-980/35 rechts right 250 R4 extrastark x-large 31.5 16 13 10
128-977/35 links left 250 L2 normal medium 27.5 14 11 8
128-979/35 links left 250 L3 stark large 29.5 15 12 9
128-981/35 links left 250 L4 extrastark x-large 31.5 16 13 10
128-982/35 rechts right 300 R2 normal medium 27.5 14 11 8
128-984/35 rechts right 300 R3 stark large 29.5 15 12 9
128-986/35 rechts right 300 R4 extrastark x-large 31.5 16 13 10
128-983/35 links left 300 L2 normal medium 27.5 14 11 8
128-985/35 links left 300 L3 stark large 29.5 15 12 9
128-987/35 links left 300 L4 extrastark x-large 31.5 16 13 10
128-988/35 rechts right 350 R2 normal medium 27.5 14 11 8
128-990/35 rechts right 350 R3 stark large 29.5 15 12 9
128-992/35 rechts right 350 R4 extrastark x-large 31.5 16 13 10
128-989/35 links left 350 L2 normal medium 27.5 14 11 8
128-991/35 links left 350 L3 stark large 29.5 15 12 9
128-993/35 links left 350 L4 extrastark x-large 31.5 16 13 10

10|
1/4
Instrumente
Mit der Hohlmeißelzange und/oder dem langen Meißel wird der laterale Erker des Acetabulums bzw. das
Os iliium für den Sattel gemuldet.
The lateral acetabular rim of the ilium is notched for the saddle using the bone rongeur and/or a long osteotome.
15-8010/07
Hohlmeißelzange n. Ruskin, modifiziert, zum
schrittweisen Öffnen des Acetabulumbodens für
das mediale Horn des Sattels, 285 mm
Ruskin rongeur, modified for gradual opening of
the acetabular floor to take the medial horn of the
saddle, 285 mm
75-3610/20
Hohlmeißel n. Dahmen, extralang,
20 mm breit, 300 mm lang
Dahmen gouge, extra-long,
20 mm wide, 300 mm long
15-1074
Hohlmeißel, gerade, 5 mm breit, 230 mm lang
Gouge, straight, 5 mm wide, 230 mm long
15-1075
Hohlmeißelzange, übersetzt, 235 mm
Bone rongeur, double action, 235 mm
15-8009
Raspatorium, retrograd gebogen, 205 mm
Raspatory, retrograde curved, 205 mm
Zum Verschieben der intrapelvinen Weichteile nach
kranial, ventral und dorsal.
To displace the intrapelvic soft tissues craniad,
ventrad and dorsad.
|11
Index Systembeschreibung
System Description
Indikationen/
Kontraindikationen
Indications/
Contraindications
Implantate
Implants
OP-Technik
Surgical Technique
Zubehör
Accessories
Literatur
Literature
Index
Index
Instrumente
Instruments
Instruments
The Lambotte osteotomes 15-2574/04 and 15-1574/06 and the gouge 15-1074 are used to open the floor
of the acetabulum step by step. The inner and outer cortical bone at the centre of the original acetabular
floor is carefully perforated to accommodate the medial saddle horn.
Mit den Lambottemeißeln 15-2574/04 und 15-2574/06 und
mit dem Hohlmeißel 15-1074 kann man den Boden des Ace-
tabulums schrittweise öffnen. Dabei durchbricht man vorsich-
tig die innere und äußere Kortikalis im Zentrum des Bodens
des ursprünglichen Acetabulums. Dies ist zur Aufnahme des
medialen Sattelhorns nötig.
15-8010/05
Aufschlaginstrument für Basisteil zur
Sattelkomponente, 220 mm
Impactor for saddle base component, 220 mm
15-8010/06
Polyethyleneinsatz für 15-8010/05, einzeln
Replacement head for 15-8010/05, single
15-2550
Schraubendreher für Sicherungsschraube
(Sattel) und Sicherungsmadenschraube
(Basisteil), 210 mm
Screwdriver for fixation screw (saddle) and set
screw (base component), 210 mm
317-720/05
Fasszange für M5 Schrauben, 160 mm
Holding forceps for M5 screws, 160 mm
Die Fasszangen zum Halten der Madenschrauben
haben in der Zangenspitze ein weibliches Gewin-
de, mit dem die jeweilige Schraube gefasst werden
kann. Man kann dann mit der Zange die Schraube
an den Einsatzort bringen und die Schraube im ge-
fassten und angelegten Zustand durch das Zangen-
modul hindurch in das Schraubenloch eindrehen.
The holding forceps for holding the set screws have a
female thread at the tip. This enables the surgeon to
position and screw in the screw while holding it with the
holding forceps.
15-8006/03
Bohrbuchse für
Spiralbohrer Ø 3 mm
Drill sleeve for twist
drill, dia. 3 mm
15-8005/03
Spiralbohrer,
Ø 3 mm, 60 mm
Twist drill,
dia. 3 mm, 60 mm
Lambottemeißel, abgesetzt, 250 mm
Lambotte osteotome, offset, 250 mm
Art.-Nr.
Item no
Breite/Width
(mm)
15-2574/04 4
15-2574/06 6

12|
OP-Technik
Die Knochenverluste im Becken sind hauptsächlich
in folgende Typen zu unterteilen:
1. Dysplasie
2. Protrusion
3. Resektion
Der Knochenverlust in der Dysplasie beruht meist
auf kraniolateraler Wanderung oder Ausbruch einer
künstlichen Pfanne. Beim Protrusionstyp wird der
Knochenverlust ebenfalls durch kraniomediale
Wanderung hervorgerufen. Dabei gibt es sowohl die
zum Beckeninneren abgegrenzte als auch die offene
Protrusion. Knochendefekte, die eine offene Protru-
sion mit Unterbrechung der vorderen und hinteren
Verbindung darstellen, resultieren meist aus Tumor-
resektionen (Abb. D).
The different types of bone loss in the pelvic region
can be broadly classified as follows:
1. Dysplasia
2. Protrusion
3. Resection
In dysplasia, bone loss is generally due to cranio-
lateral migration or loosening of an artificial acetabular
component. In the protrusion type, bone loss may
also be caused by craniomedial migration. It should
be noted that protrusion may be either separated
from the inner pelvis or open. Bone defects charac-
terised by an open protrusion, with an interruption of
the anterior and posterior connection, are usually the
result of tumour resection (Fig. D).
Allgemeines General
Abb./Fig. D

|13
Index Systembeschreibung
System Description
Indikationen/
Kontraindikationen
Indications/
Contraindications
Implantate
Implants
Instrumente
Instruments
Zubehör
Accessories
Literatur
Literature
Index
Index
OP-Technik
Surgical Technique
Surgical Technique
Grundsätzlich sollte man die Länge des Basisteils
so wählen, dass die Reposition bei genügender
Spannung durch die verbliebenen, das Gelenk
überbrückenden Weichteilstrukturen, durchgeführt
werden kann. Durch diese Weichteilspannung ist ein
Schutz gegen mögliche Luxation gegeben.
In der Revisionsarthroplastik werden vorwiegend
kurze Basisteile verwendet, wobei die Reposition
wegen der Narben im Weichteilgewebe häufig
Schwierigkeiten bereiten. Hingegen werden in der
Knochentumorchirurgie eher die längeren Basisteile
Anwendung finden, da das Artikulationsniveau meist
höher liegt und die Spannung in den nach Resektion
verbliebenen Normalmuskeln meist gering ist. Dann
ist auch eine Beinverlängerung in Kauf zu nehmen.
Besteht ein erhöhtes Luxationsrisiko, was man
gegebenenfalls durch intraoperative Prüfung her-
ausfindet, limitiert man eventuell für einige Wochen
kritische Bewegungen. Gegebenenfalls wird der
Patient durch leichte Traktion oder nach Wundhei-
lung mittels Gipshose immobilisiert.
Wenn sich später nach einigen Wochen um das
Sattelgelenk eine bindegewebsartige Pseudokapsel
gebildet hat, die dann weiterhin auch noch verknö-
chert, ist die Luxationsgefahr nur noch gering.
Kommt es allerdings zur Luxation, muss häufig offen
reponiert werden, da der Sattel sich beim Versuch
der geschlossenen Reposition verdreht, wenn das
mediale Horn den Knochen berührt.
Bei der Befestigung der Sattelkomponente auf
einem Basisteil ist darauf zu achten, dass die Si-
cherungsschraube, die den Sattel auf dem Basisteil
sichert, von lateral eingesetzt wird, so dass sie für
eine eventuelle Reoperation gut zugänglich ist.
Generally speaking, the chosen base component
length should facilitate reduction by working with
the remaining soft-tissue structures, given sufficient
tension. This type of soft-tissue balancing helps
reduce the chance of dislocation.
In revision arthroplasty, short base components are
used in most cases and soft-tissue scarring often
poses a problem for reduction. In contrast, in bone-
tumour surgery, the longer base components tend
to be used, since the articulation level is generally
higher and there is usually little tension in the normal
muscles that remain after resection; leg lengthening
may be unavoidable. If the patient has a high risk of
dislocation – this evaluation may be done intraope-
ratively – it may be necessary to limit critical move-
ments for a few weeks. If necessary, the patient
is immobilised by applying either light traction or a
Whitman’s plaster after the wound has healed.
The risk of dislocation becomes minimal once a
fibrous pseudocapsule has formed around the
saddle joint after a few weeks, which then continues
to ossify.
If, however, dislocation does occur, an open re-
duction is nearly always required, since the saddle
twists when a closed reduction is attempted and
the medial horn makes contact with the bone.
When attaching the saddle component to the base
component, it is important to ensure that the fixation
screw, which fixes the saddle to the base component,
is inserted from lateral so that it is accessible in the
event of revision.
14|
OP-Technik
Bei der Dysplasie ist der kraniolaterale Wulst des
Acetabulums nicht mehr vorhanden. Der Acetabu-
lumboden ist üblicherweise geschlossen.
Zum Einstellen des Sattels muss er deshalb geöffnet
werden. Danach benutzt man das dreieckige retro-
grad gewinkelte Raspatorium, um die intrapelvinen
Weichteile nach kranial, ventral und dorsal zu ver-
schieben. Dann ist das Acetabulum derart zu
resezieren, dass dorsale Knochenstrukturen, die die
Schwenkbewegungen des Sattels eventuell stören
könnten, entfernt werden. Beim Dysplasietyp liegt
der Artikulationsbereich des Sattels meist eher medial.
In dysplasia, the craniolateral acetabular rim is no
longer present. The floor of the acetabulum is usually
closed and, therefore, needs to be opened in order to
introduce the saddle. The triangular retrograde angled
raspatory is then used to displace the intrapelvic soft
tissues craniad, ventrad and dorsad. The acetabulum
must then be resected so that any dorsal bone
structures which could impede saddle pivoting are
removed. In the dysplasia type, the area of saddle
articulation tends to be medial.
Spezielles: Dysplasietyp Specifics: Dysplasia Type

|15
Index Systembeschreibung
System Description
Indikationen/
Kontraindikationen
Indications/
Contraindications
Implantate
Implants
Instrumente
Instruments
Zubehör
Accessories
Literatur
Literature
Index
Index
OP-Technik
Surgical Technique
Index Systembeschreibung
System Description
Indikationen/
Kontraindikationen
Indications/
Contraindications
Implantate
Implants
Instrumente
Instruments
OP-Technik
Surgical Technique
Zubehör
Accessories
Literatur
Literature
Index
Index
Surgical Technique
Liegt eine Protrusion vor, so muldet man den in der
Regel erhaltenen lateralen Wulst des Acetabulums
als Gegenlager für die Artikulation mit dem Sattel
aus. Ist der intrapelvine Bereich durch eine (meist
dünne) Knochenlamelle abgegrenzt, ist diese zu
durchbrechen, so dass man das mediale Horn des
Sattels in das Becken einstellen kann. Dabei ist
abzusichern, dass das Sattelhorn nicht zwischen
innerer und äußerer Kortikalis angeordnet wird. Bei
Protrusionen, die häufig keine derartige Abgrenzung
aufweisen, muldet man lediglich den acetabulären
Wulst, falls dies überhaupt noch nötig ist. Auch hier
werden die kaudalen Knochenanteile, die die Sattel-
beweglichkeit möglicherweise behindern, entfernt.
Die Sattelartikulation ist beim Protrusionstyp meist
etwas lateralisiert.
In the case of protrusion, the lateral acetabular rim,
which is generally preserved, is notched to form a
bearing surface for saddle articulation. If the intra-
pelvic area is separated by a (generally thin) lamella
of bone, the latter must be perforated to accommo-
date the medial horn of the saddle within the pelvis.
It is important to ensure that the saddle horn is not
located between the inner and outer cortical bone.
In the case of protrusions without such separation,
only the acetabular rim is notched, if necessary.
Any caudal bone portions that could impede saddle
mobility are removed in this case too. In the protru-
sion type, the site of saddle articulation is generally
more lateral.
Spezielles: Protrusionstyp Specifics: Protrusion Type

16|
OP-Technik
Die Nachbehandlung erfolgt ähnlich wie bei der
totalen Hüftgelenkprothese. So werden am ersten
postoperativen Tag isometrische Muskelspannungs-
übungen sowie Drehbewegungen in den Fußgelenken
und zusätzlich Atemübungen durchgeführt.
Nach Entfernung der Saugdränagen und Verband-
wechsel darf der Patient dann unter krankengym-
nastischer Hilfestellung aufstehen und im Gehwagen
seine ersten Schritte durchführen. Das operierte Bein
kann dabei belastet werden. Es folgt die weitere
Mobilisation durch krankengymnastische Bewegungs-
übungen mit Gehwagen, Unterarmstützen und
Handstöcken, wobei die Anwendung der Stützmittel
eher großzügig und bei Unsicherheit des Patienten
langfristig vorzusehen ist. Besonders in Tumorfällen
mit großen Resektionen ist zu entscheiden, ob eine
Bewegungslimitierung oder gar Immobilisation für
gewisse Zeit nötig ist.
After-treatment is similar to that for total hip prostheses.
The patient does isometric muscle contraction, foot
rotation and breathing exercises on the first postope-
rative day. Once the wound drainage devices have
been removed and the dressings changed, the
patient may stand up with the assistance of a physical
therapist and take his first steps with the aid of a walker,
at which point he may put weight on the operated leg.
Mobilisation proceeds with physio-therapy exercises
with the aid of a walker, elbow crutches or cane.
Plenty of support should be provided – long-term if
the patient shows unsteadiness. In tumour cases
involving extensive resection in particular, it must be
determined whether restriction of movement or even
immobilisation is necessary for a time.
Bei vorliegender Knochenresektion muldet man die
untere Kante des Os iliium etwa entsprechend der
Höhe des Sattelzentrums. Um die Mulde im Ilium
herzustellen, eignen sich besonders die Hohlmeißel-
zange 15-1075 und der extralange Hohlmeißel nach
Dahmen 75-3610/20.
In the resection type, the inferior margin of the ilium
is notched to the approximate depth of the saddle
centre. The bone nibbling rongeur 15-1075 and the
extra-long Dahmen gouge 75-3610/20 are ideal for
notching the ilium.
Spezielles: Resektionstyp Specifics: Resection Type
Postoperative Behandlung Postoperative management

|17
Index Systembeschreibung
System Description
Indikationen/
Kontraindikationen
Indications/
Contraindications
Implantate
Implants
Instrumente
Instruments
Zubehör
Accessories
Literatur
Literature
Index
Index
OP-Technik
Surgical Technique
Surgical Technique
Dysplasietyp
66-jährige Patientin, bei der wegen einer Dysplasie-
coxarthrose 1969 rechts und 1972 links totale Hüft-
gelenkendoprothesen implantiert wurden.
Wegen zwischenzeitlicher Lockerung links war 1988
eine Austauschoperation erforderlich. 1989 zeigte
sich ein erneutes grobes Versagen des linken
Kunstgelenkes der Hüfte.
1989 wurde das linke Kunstgelenk der Hüfte revi-
diert. Es wurde eine Austausch-OP durchgeführt.
Aufgrund erheblicher knöcherner Destruktionen
der Pfannenanlage des Dysplasietyps wurde eine
Sattelendoprothese implantiert.
Nach einer gesetzten Perforation des Knochens
wurde der Sattelkopf an der Beckenschaufel ab-
gestützt. Über ein Basisteil Nr. 1 erfolgte die Ver-
bindung zu einer Schaftprothese Endo-Modell®
Schaftstärke 5.
1990 zeigte sich nach geringgradiger Migration des
Sattelkopfes nach kranial eine gute beginnende
Sklerosierung im Belastungsbereich an der Becken-
schaufel.
1995: Zunahme der Sklerosierung im Belastungs-
bereich des Sattelkopfes. Das mediale Knochen-
horn ist vollständig im knöchernen Gleitlager einge-
bettet.
Dysplasia type
A 66-year-old female patient who, due to dysplastic
coxarthrosis, received a total hip replacement on
the right in 1969 and on the left in 1972.
Revision surgery on the left was performed in 1988
due to loosening. In 1989, the left hip replacement
showed major failure again.
The left hip replacement was revised in 1989;
an exchange operation was performed. A saddle
prosthesis was implanted due to severe destruction
of the acetabular bone stock resulting from dysplasia.
After the bone had been perforated, the head of the
saddle was supported on the iliac wing. The saddle
was connected to an Endo-Model® femoral stem
size 5 via a no. 1 base component.
In 1990, there was evidence of good incipient scle-
rosis in the weight-bearing area of the iliac wing
following slight craniad migration of the saddle head.
By 1995, the progression of sclerosis in the weight-
bearing area of the saddle head was such that the
medial horn was completely embedded in the bony
bearing.
Fallbeispiele Case Histories
18|
Protrusionstyp
Bei einem 72-jährigen Patienten, dem 1975 wegen
einer Coxarthrose rechts eine totale Hüftgelenkpro-
these implantiert wurde, erfolgte 1983 aufgrund einer
periprothetischen Infektion eine Austauschoperation.
Danach musste die Pfanne wegen Lockerung zweimal
gewechselt werden.
Nochmalige Pfannenlockerung mit Destruktion der
Pfannenanlage und Protrusion.
1988 erfolgt eine Revision des rechten Hüftgelenks
mit einer 200 mm langen Revisionsprothese, auf die
ein mittellanges Basisteil mit Sattel gesetzt wurde.
Beim Protrusionstyp muldet man die in der Regel
erhaltenen lateralen Erker des Acetabulums zur Arti-
kulation mit dem Sattel. Ist das Innere des Beckens
durch eine dünne Knochenlamelle abgegrenzt, muss
man diese durchbrechen, damit das mediale Horn
des Sattels im Becken liegt. Bei offener Protrusion
muldet man den Erker, falls nötig.
Seit 1992 unveränderte Stellung des Sattels zum
Becken mit guter Sklerosierungszone.
Protrusion type
A 72-year-old male patient had received a right total
hip replacement in 1975 due to coxarthrosis.
A revision was performed in 1983 following peri-
prosthetic infection. It was subsequently necessary
to replace the acetabular component twice due to
loosening.
The patient again showed loosening of the aceta-
bular component, accompanied by destruction of
acetabular bone stock and protrusion.
In 1988, revision surgery was performed on the right
hip using a 200 mm-long revision stem, on which a
medium-length base component with saddle was
mounted.
In the protrusion type, the lateral acetabular rim, which
is generally preserved, is notched for saddle articu-
lation. If the inner pelvic area is separated by a thin
lamella of bone, the latter must be perforated to
accommodate the medial horn of the saddle within
the pelvis. In the case of open protrusions, the ace-
tabular rim is notched, if necessary.
Since 1992, the position of the saddle in relation to
the pelvis has remained unchanged, with a good
zone of sclerosis.
OP-Technik
This manual suits for next models
17
Table of contents

















