45
4. traumatic—TBI, stroke, surgery
5. fibromyalgia--chronic pain, chronic fatigue
6. insomnia
7. peak performance
8. misc: Parkinsons and other tremors
Setting Apropos Expectation
. Assist clients in establishing appropriate expecta-
tions for the session, that it is a process. Help them real-
ize that situational occurrences like a death of a loved
one, or a traumatic brain injury or illness or emotion-
al trauma that’s recently occurred, may be swifter to
resolve, while longer standing issues may take time.
The Essential Observation Sheet
. Always urge the criticalness and explain the
significant value of the “Observation Sheet.” The patient/
client must commit to being a participant in their own
healing process. Without this they will look to you for
only one reason: to fix them.
Show Them You “See” Them
. Review their Observation Sheet results at the
beginning of each and every session to reward them for
being a participant in their own process, and showing
a commitment to their healing. It shows them your
support and helps them feel “seen” and empathically
understood. Be their “cheerleader and inspiration,” after
all, they chose you for that reason ultimately.
The Initial Assessment
. Always refer back to the initial assessment in
order to choose the appropriate protocol. While their
symptoms are reducing, and their CNS is permanently
very different from session to session, we don’t want to
overestimate the patient/client’s system and progress
when contraindicated.
The 10/20 Site Pairing
. In 90% of the cases you treat, expect to utilize
various site pairs from the 10/20 site pairing on the
“Genesis” Protocol on the first session. The more
challenging discussion here is what to do and when
to do so for the remaining 10%. While the following
breakdown is open to some interpretation which we
welcome you to discuss with us when in doubt, as a
set of Standards of Care, we request that you carefully
follow these guidelines.
Choosing from the 10/20 Site Pairings
. Measures of Reactivity in Selecting Protocols and
Site Pairings on session #1 (When the measures of
reactivity indicate definite issues):
• 0-1 issues of concern of the measures of re-
activity: 4-5 of the 10/20 site pairing on Genesis
• 2 issues of concern of the measures of
reactivity: utilize 4 of the 10/20 site pairing on
Genesis (depending on acuity; the higher the
acuity, the lower number of site pairs, especially
in the case of seizure potential)
• 3
is-
sues
of
concern
of the
measures
of reactiv-
ity: utilize 3-4
of the 10/20 site
pairing on Genesis
(depending on acuity;
the higher the acuity,
the lower number of site
pairs, especially in the case
of seizure potential)
• 4+ issues of concern of the
measures of reactivity: utilize 1-3
of the 10/20 site pairs on Genesis
(depending on acuity; the lower num-
ber of site pairs, especially in the case of
seizure potential)
If a person is overstimulated: mildly – reduce by ½;
significantly – reduce by 2/3 or more.
. Seizure Potential
IASIS does not lead to seizures in patients without
a seizure history. If there is any potential to trigger a
seizure in someone with uncontrolled seizures, IASIS
should not be done. There is a difference between
true seizures and pseudo-seizure but most clinicians
including MDs can’t tell the difference. Only epilep-
tologists have the expertise to do so, and it is firmly in
the IASIS Guidelines of Care that patient/clients with
epilepsy be exclusively under the care of highly trained
medical professionals.
. When in Doubt – DON’T
Even if you think you should do something different
because of what a patient/client has told you; and
especially if the patient/client has said, “Hey, look,
this isn’t moving as quickly as I’d like it to, so can we
please move it along and make it stronger?” We say,
“no we cannot, we have Guidelines of Care that are
designed to keep you safe and proceed accordingly.
You wouldn’t want to take a chance, would you? I will
not.”
Examples of overstim: tired, wired, spacey, headache,
nausea, or the exacerbation of symptom(s). Be par-
ticularly careful with spaciness when one must drive
after sessions as this may present danger when driving.
This is our strongest tenet of our Guidelines of Care.
While IASIS is not considered by most as a medical
treatment, we still hold as our highest goal and
boundary, “harm to none.”
IASIS MCN is working on the parasympathic and sym-
pathetic nervous system, sometimes referred to as the
“accelerator” and the “brake”.
Differences between IASIS MCN and traditional neu-
rofeedback: micro stimulation versus feedback, dis-
entrains versus trains the brain, passive versus active.
Working with Fragile/Reactive Patients
. After the initial session, if one site pair was
utilized, and from the Observation Sheet, little to no
measures of reactivity were reported, a second site pair
may be added. Again, with each additional session, you
may choose to add additional site pairs, so long as no
significant measures of reactivity are reported. Keep in
mind that if four or five site pairs or more are getting a
positive response, there may be no reason to increase
the number of site pairs of cycles. More is not better.
After the Initial Session
. Subsequent IASIS sessions after the initial session
for potentially fragile/reactive patients/clients will vary
widely depending on the feedback you receive as to
how an individual responds/reacts.
As sessions continue and Observation Sheet reports
roll in demonstrating diminished anxiety, reactivity and
impulsivity, numerous other issues are lessened and
better regulated sleep may be reported (for example),
one may increase the number of site pairs, still cogni-
zant of the initial assessment. Remember the constitu-
tion of the patient/client. Use great caution not to be
falsely lulled into imagining that because of a reduction
in symptoms, they’ve developed a hardy CNS.
Remember to look at their constitution and posture
and body language. Be sure you remind them to have
food and water before coming in since it’s believed neu-
rotransmitter changes are occurring and they may be
a bit more relaxed than normal. They may wish to have
someone drive them in fact. Other family members
often notice the greatest changes.
Also keep in mind that the greatest changes occur when
one is deepest down the rabbit hole of their condition.
Again, for some, fewer site pairings may be just right.
Less is always more as with homeopathic remedies.
Remind your patients/clients that an effective IASIS ex-
perience is dependent on “reach and frequency” – the
ability of IASIS to mediate its effects on the CNS over
a period of time. In many cases it took years for the
person to get to their current state. It stands to reason it
may take a while to see a turnaround in their condition.
It’s ultimately a serious endeavor, a balance that is part
art, and part science.
Hormesis in Daily Life
. Several articles describe evidence supporting
hormesis as a mechanism responsible for the health
benefits of a variety of lifestyle and environmental
factors. This is best documented for exercise which
increases the resistance of musculoskeletal and car-
diovascular systems to injury and disease (Kojda and
Hambrecht, 2005). But moderate regular exercise also
benefits other tissues including the nervous system
(Gomezi-Pinilla, 2007) and digestive system (Bi and
Triadafilopoulos, 2003). Zsolt Radak and Fernando
Gomez-Pinilla cover the current state of knowledge of
the hormetic effects exercise on muscle and nerve cells
(Gomez-Pinilla, 2007; Radak, 2007).
The public in industrialized countries is bombarded
with a bewildering array of information on the effects
of dietary factors on health (Satia-About a et al., 2002).
However, the only well-established means of improv-
ing health through diet is maintaining a relatively low
caloric intake, as described previously (Masoro, 2005;
Martin et al., 2006). An article in this issue of ARR de-
scribes the involvement of hormesis mechanisms in the
beneficial effects of dietary energy restriction on health,
and also highlights emerging evidence supporting a
role for hormesis in the health-promoting actions of
several widely-studied chemicals in fruits and vegeta-
bles (Mattson, 2007).
Accumulating evidence suggests that the reason that
regular engagement in intellectual activities is benefi-
cial for the brain (Scarmeas and Stern, 2003) is that it
activates hormetic pathways in neurons. Similar to the
changes that occur in muscle cells during exercise,
neurons engaged in challenging activities are sub-
jected to repeated bouts of calcium influx, free radical
production and moderate (aerobic) energetic stress
(Mattson et al., 2002; Serrano and Klann, 2004). As a
result, transcription factors such as cyclic AMP response
element binding protein (CREB) and nuclear factor kB
(NF-kB) are activated (Carlezon et al., 2005; Mattson
and Meffert, 2006), and the expression of several major
classes of cytoprotective proteins is increased including
neurotrophic factors, heat-shock proteins and others
(Lazarov et al., 2005).
As with other organ systems, exposure of the cells in
the nervous system to mild and transient bouts of
stress may increase their resistance to the adversities
of ageing. Suresh Rattan reviews the role of hormesis
mechanisms in modifying the ageing process in this
issue of ARR (Rattan, 2007).
Hormesis Article Nih: https://www.ncbi.nlm.nih.gov/
pmc/articles/PMC2248601/pdf/nihms39393.pdf
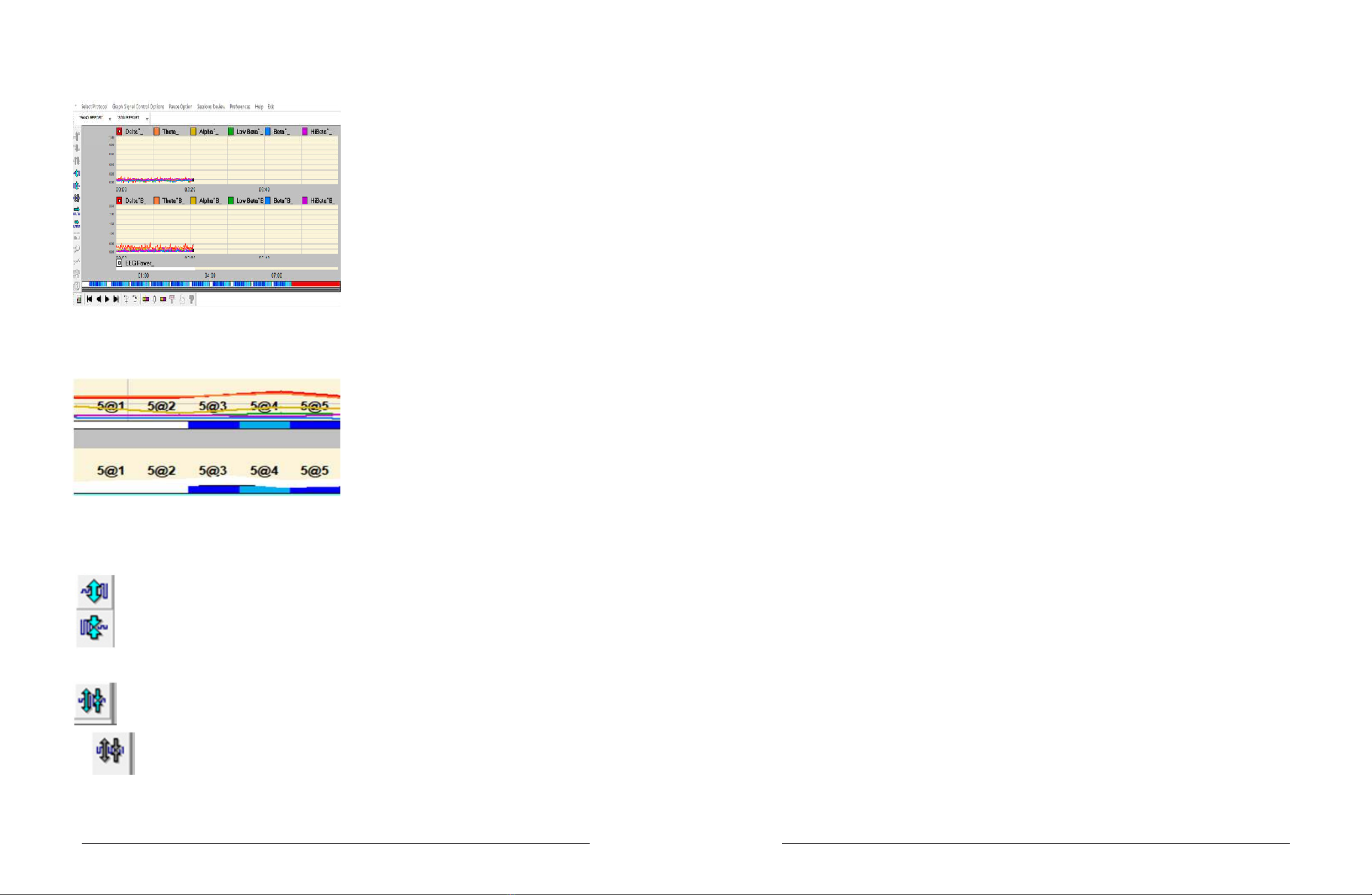
Micro Dose Protocol
.The following protocol is to be considered where
extreme reactivity or significant potential fragility in the
CNS exists.
• Protocol = Genesis
• Site Pairs = 3 (F3/F4, F7/F8, NZ/OZ)
• 5 seconds system on and operating; 2 seconds off,
(3 exposures at a 5 second duration per Site Pair)
Barry Bruder - IASIS Technologies, Inc.
© 2013-2019