VORTRAN®Medical 5/26/2017
VORTRAN®GO2VENT™ User’s Guide
Page4
II. Clinical Considerations (continued)
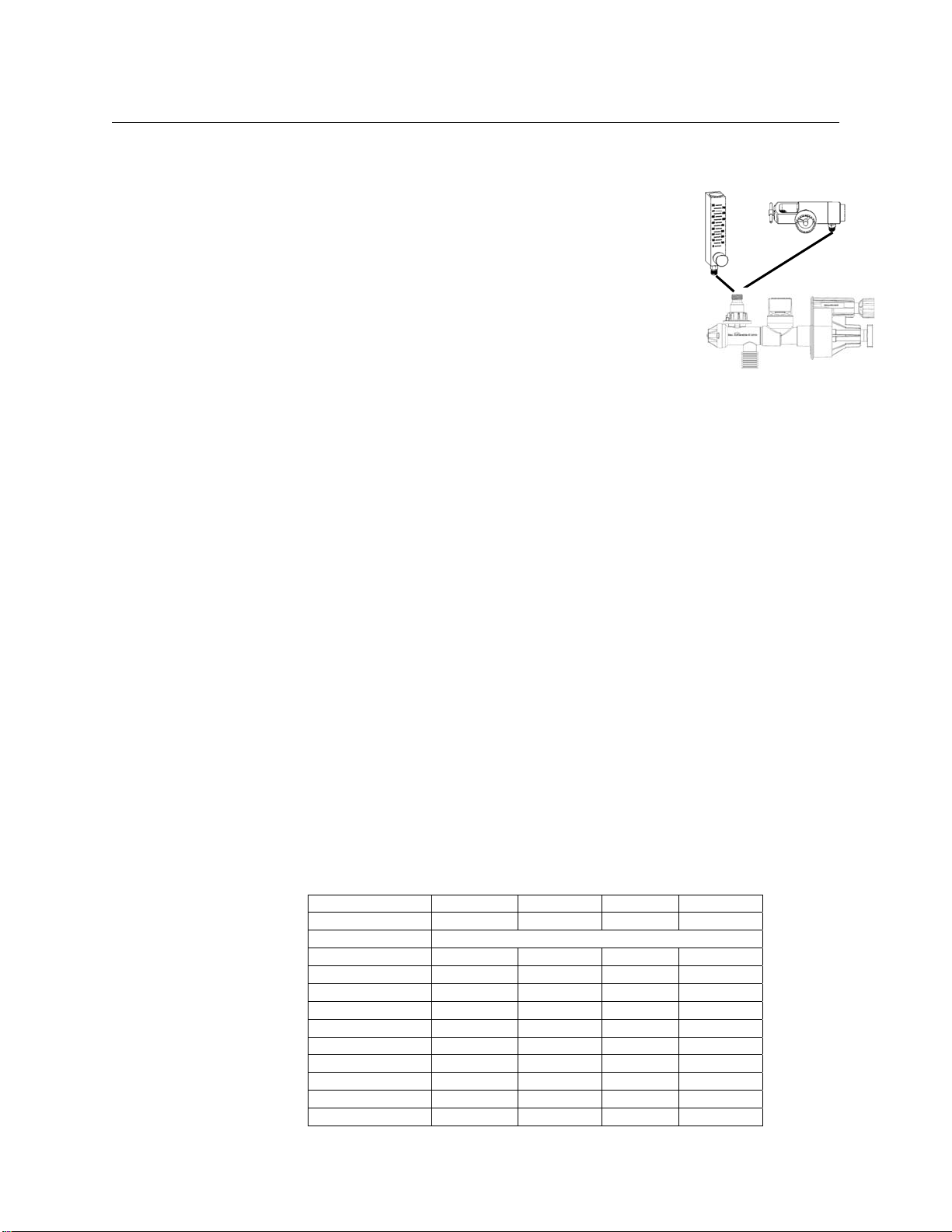
The GO2VENT™runs on a continuous gas flow (inspiratory flow) of 6 to 40 L/min
depending on patients’ inspiratory flow demand. When connected to a 50 PSIG
gas source, the GO2VENT™will automatically deliver 40 L/min (667 mL/second)
per ASTM Guideline1. Delivered tidal volume may be determined by multiplying
the flow in mL/second and the inspiratory time in second, or by using the
estimated tidal volume table.
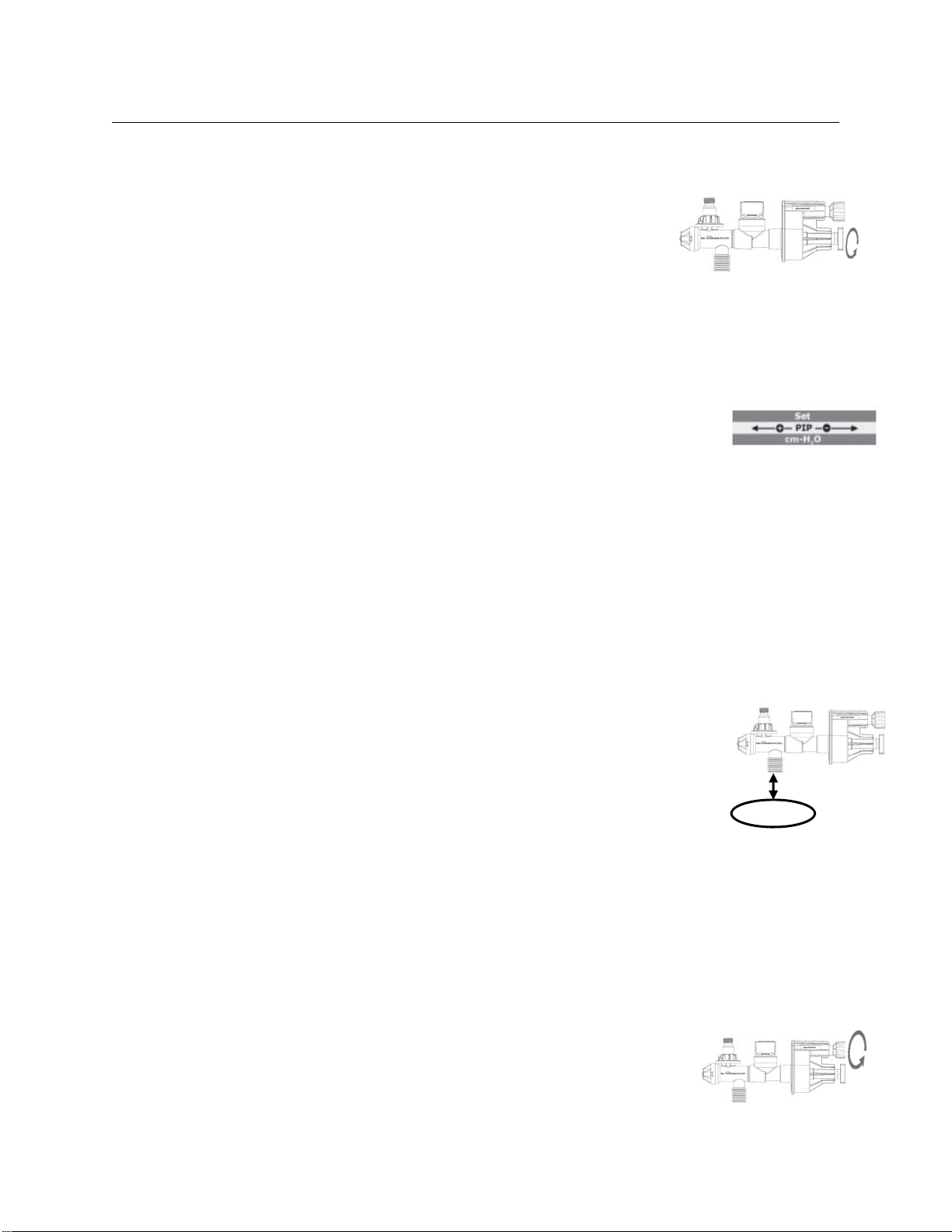
The rate dial controls exhalation time (texhl), and when dialed down enough will
cause the GO2VENT™ to stop cycling automatically (infinite exhalation time).
Under these circumstances, the GO2VENT™ is delivering pressure supported
ventilatory support and the patient must trigger the GO2VENT™ to begin
subsequent full inhalations. If the patient is apneic or pressure control
ventilation is desired, restart automatic cycling of the GO2VENT™ by adjusting
the rate dial counterclockwise until cycling begins again. Whenever the
GO2VENT™stops cycling, the first step in the absence of obvious clinical factors,
is to check if it is in pressure support mode by rotating the rate dial counter
clockwise (out). If rotating the rate dial counter clockwise substantially (3 or 4
turns) does not start automatic cycling, the patient’s airway may be occluded or
a very large leak exists.
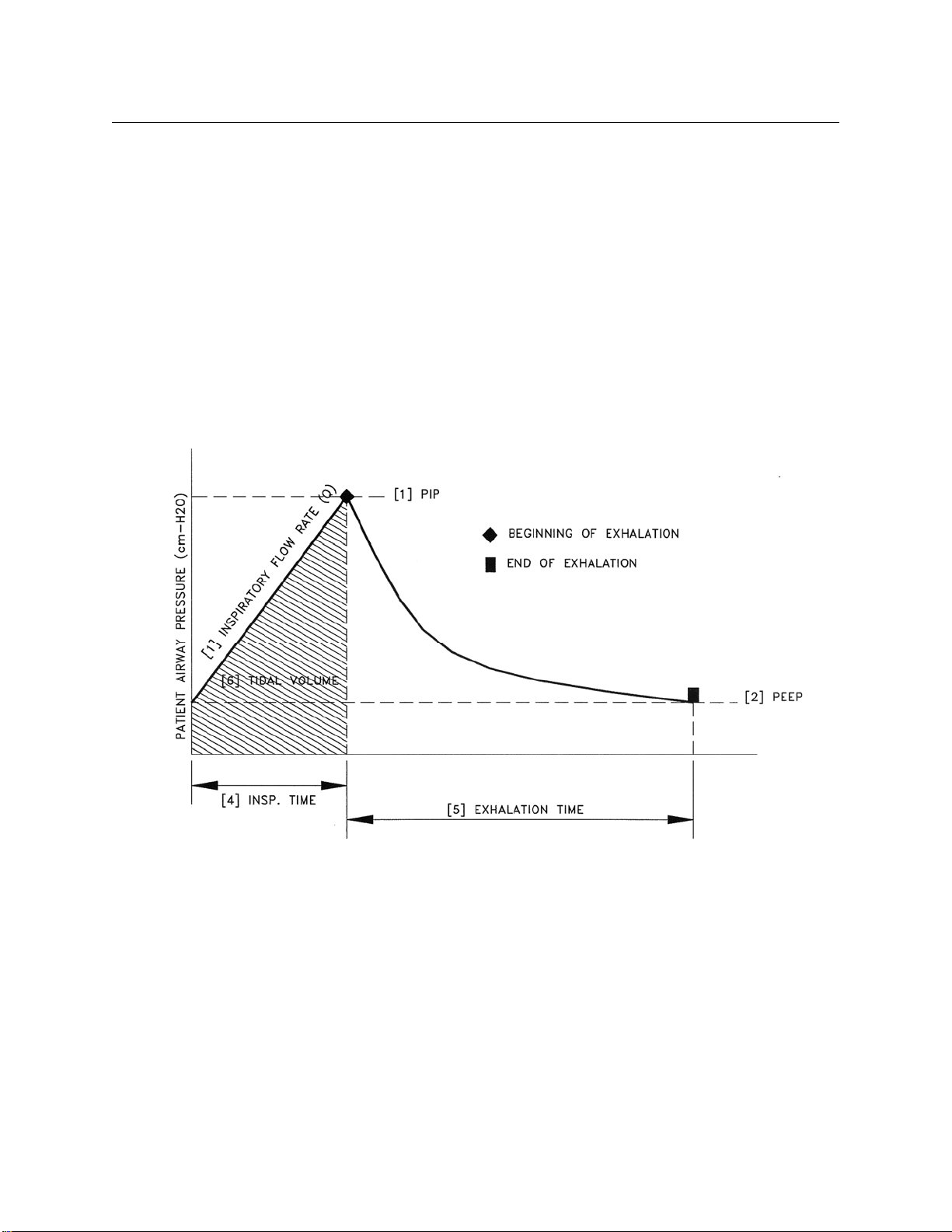
The PIP may be adjusted from 10 and 50 cm H2O. The PEEP is intrinsic to the
device which ranges from 2 to 9 centimeters and is directly proportional to the
set PIP. Inspiratory time and rate are adjustable over a wide range. Changes in
the PIP setting or flow will also affect the respiratory rate. It is important to
check all settings when making a change to any of these three variables (flow,
PIP and rate). For example: reducing the PIP setting may cause the GO2VENT™
to go into spontaneous breathing mode. Adjust the rate dial out (counter-
clockwise) to restart automatic cycling.
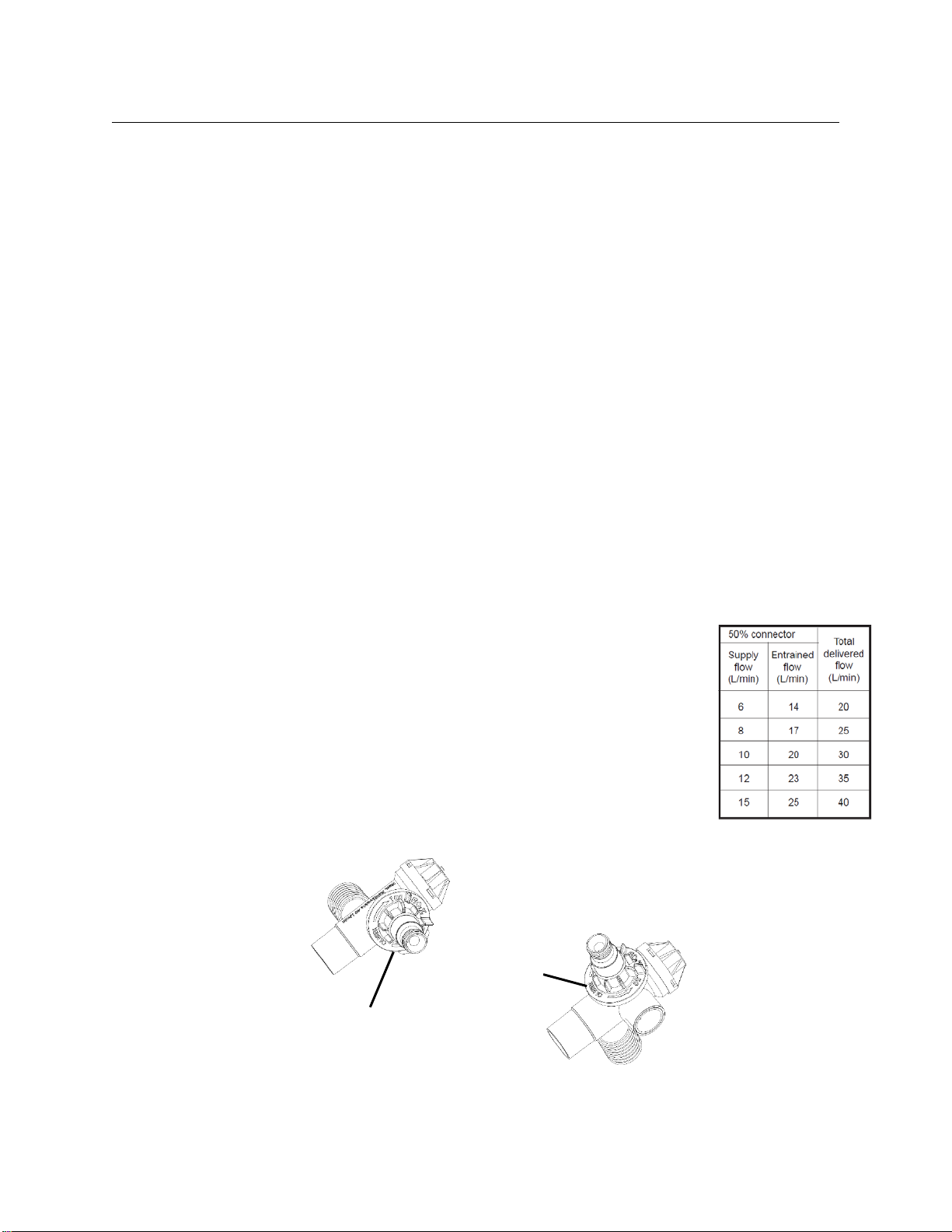
The GO2VENT™ is equipped with an air entrainment valve which allows the
patient to entrain additional air and respond to the demands of the patient.
Patient entrainment of outside air is normally audibly detectable and the percent
oxygen delivered to the patient will be reduced. Specific concentrations of
oxygen may be delivered to the patient with the use of an oxygen blender.
Although the design of the modulator is similar to that of a pop-off valve and is
inherently safe, the GO2VENT™® is also equipped with a redundant pop-off valve
that relieves pressure at 60 cm H2O. When the pop-off valve is activated, the
pop-off valve piston will be seen to open slightly and excess pressure released.
1StandardSpecificationforMinimumPerformanceandSafetyRequirementsforResuscitatorsIntendedforUsewith
Humans,ASTMDesignation:F920–93.