IMPLOX Newborn Anne Manual

T
TABLE OF CONTENTS
INTRODUCTION
Introduction and Intended Use . . . . . . . . . . . . . . . . . . . 2
SETUP GUIDE
Newborn Anne Package Contents . . . . . . . . . . . . . . . . 3
Manikin Connectors . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
CLINICAL SIMULATION
General Handling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Airway Simulation Features . . . . . . . . . . . . . . . . . . . . . . .7
Drug & IV Administration . . . . . . . . . . . . . . . . . . . . . . .10
Manikin Preparation Before Use . . . . . . . . . . . . . . . . . 11
MAINTENANCE
Maintenance After Use . . . . . . . . . . . . . . . . . . . . . . . . 12
Periodic Maintenance . . . . . . . . . . . . . . . . . . . . . . . . . . 12
ENGLISH
CLINICAL
SIMULATIONSETUP GUIDEINTRODUCTION
ENGLISH
1
MAINTENANCE
2
SETUP GUIDE
CLINICAL
SIMULATION
Newborn Anne M
Manikin
Features
Airway Features:
• Anatomically accurate, realistic airway
• ET tube insertion
• LMA insertion
• Sellick Maneuver
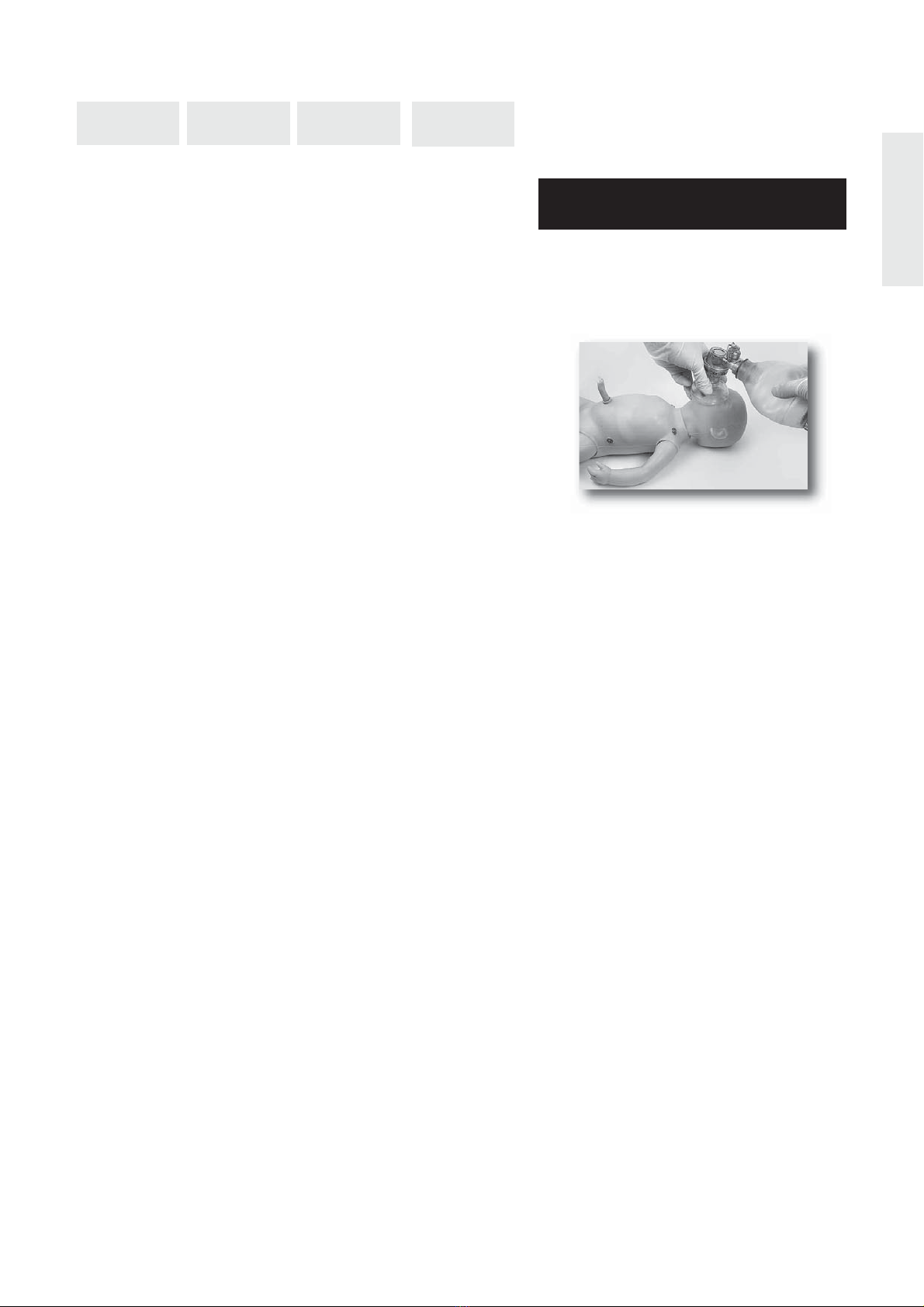
• Positive pressure ventilation
• Mainstem intubation
• Suctioning
• Gastric tube insertion
Breathing Features:
• Bilateral chest rise and fall with mechanical
ventilation
Breathing Complications:
• Unilateral needle thoracentesis - anterior-axillary
Vascular Access:
• Patent, cuttable umbilicus with venous and
arterial access for bolus or continuous infusion
• Intraosseous access – bilateral
• Simulated blood flashback upon cannulation
Other Features:
• Interchangeable pupils with normal, dilated and
constricted pupils (optional)
• Articulation in all four limbs
• Stomach reservoir
• Umbilical reservoir
• Manual umbilical pulse
INTRODUCTION
Introduction and Intended Use
MAINTENANCE
Newborn Anne
Manikin
Newborn Anne focuses on training in basic neonatal resuscitation skills.

Cat.no. Description Cat.no. Description Cat.no. Description
220-03650 Meconium Kit
220-00650 Baby Pants
250-21050 Airway Lubricant
300-00750 Red Simulated Blood
276-15550 Liquid Soap
277-00150 Baby Powder
240-01050 Carry Case
220-05550 Umbilical Pulse Bulb
220-05650 Umbilical Clamp
220-05750 IV Bag Connector Tube
220-19250 Directions for Use CD
5527 Laerdal Global Warrranty
Optional Accessories: (Not shown)
200-03050 Eye Kit
220-00350 Right & Left IO Mandrel and Leg
Skin Kit
220-00150 Umbilical Cord (4)
240-00250 Umbi Simulated Blood
220-00250 IV Bag &Tubing Set
3
ENGLISH
INTRODUCTION
CLINICAL
SIMULATION
SETUP GUIDE
Baby Pants
Newborn Anne Manikin
Umbilical Clamp
Liquid
Soap Baby
Powder
Umbilical
Cord (1)
Directions for Use
Red
Simulated
Blood
Setup Guide
Not shown:
* Laerdal Global Warranty
* Carry Case
* Meconium Kit
Airway
Lubricant
Newborn Anne Package Contents
The following parts are included in the Newborn Anne shipping carton.
MAINTENANCE
IV Bag Connector Tube
Pulse Bulb Tube

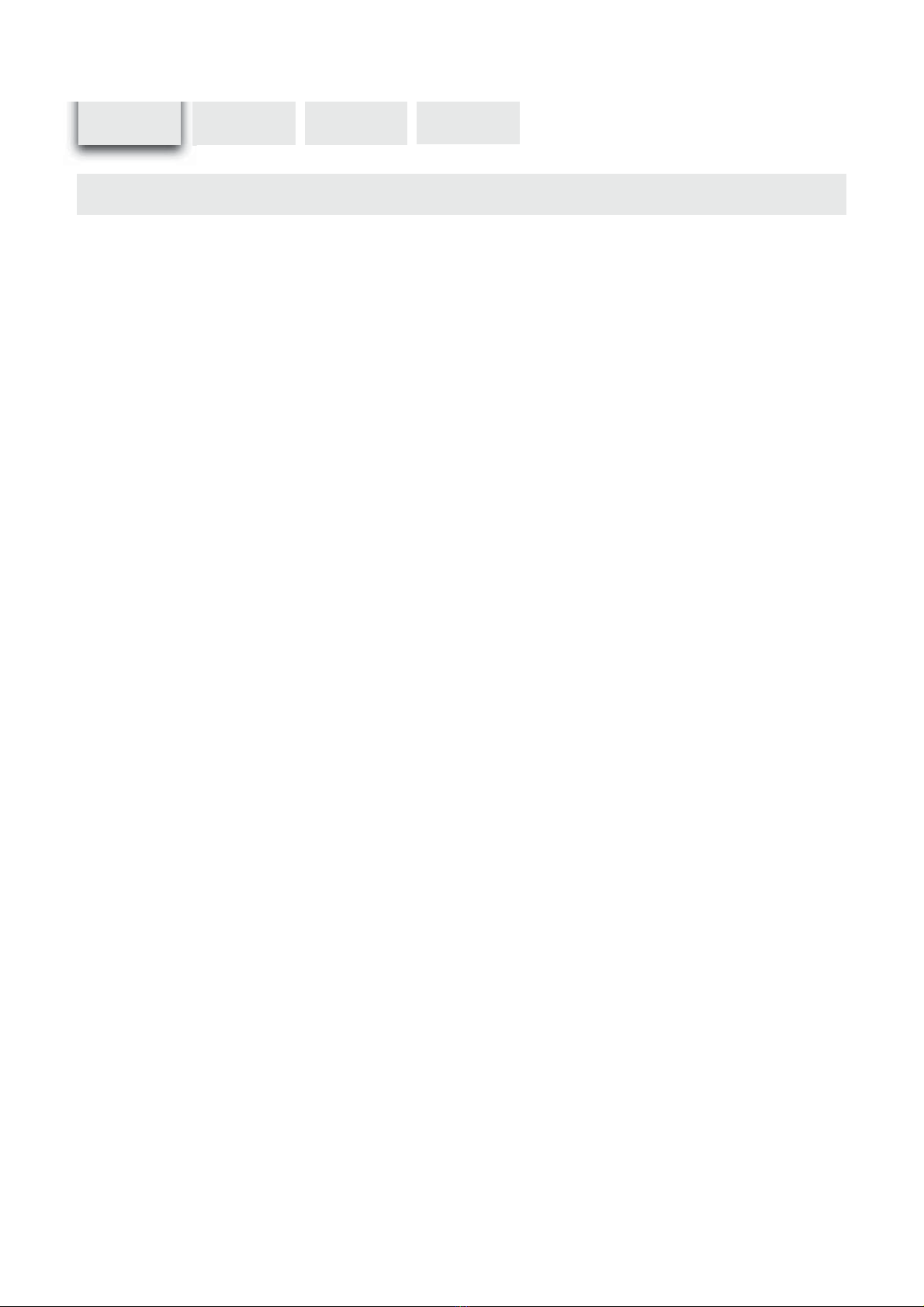
Manikin Connectors
The Newborn Anne manikin is shipped ready for use.
4
INTRODUCTION
CLINICAL
SIMULATION
DA
B
SETUP GUIDE
Note - The manikin’s Umbilical Reservoir Tube Connection (D) has a valve to prevent leakage from the tube when
not attached to an IV-bag set.
* To attach an empty IV Bag (not provided), connect the IV Bag Connector Tube (C) to the manikin’s Umbilical
Reservoir Tube Connection (D).
* To attach the Umbilical Pulse Bulb Tube (B), connect to the manikin’s Umbilical Pulse Bulb Tube Connection (A).
Note - To attach the tubes, push the connectors together and quarter turn. To detach, reverse the process.
MAINTENANCE
C
Table of contents
Other IMPLOX Medical Equipment manuals


Popular Medical Equipment manuals by other brands







Getinge
Getinge Arjohuntleigh Nimbus 3 Professional Instructions for use

Mettler Electronics
Mettler Electronics Sonicator 730 Maintenance manual

Pressalit Care
Pressalit Care R1100 Mounting instruction

Denas MS
Denas MS DENAS-T operating manual

bort medical
bort medical ActiveColor quick guide

AccuVein
AccuVein AV400 user manual





