Page 4
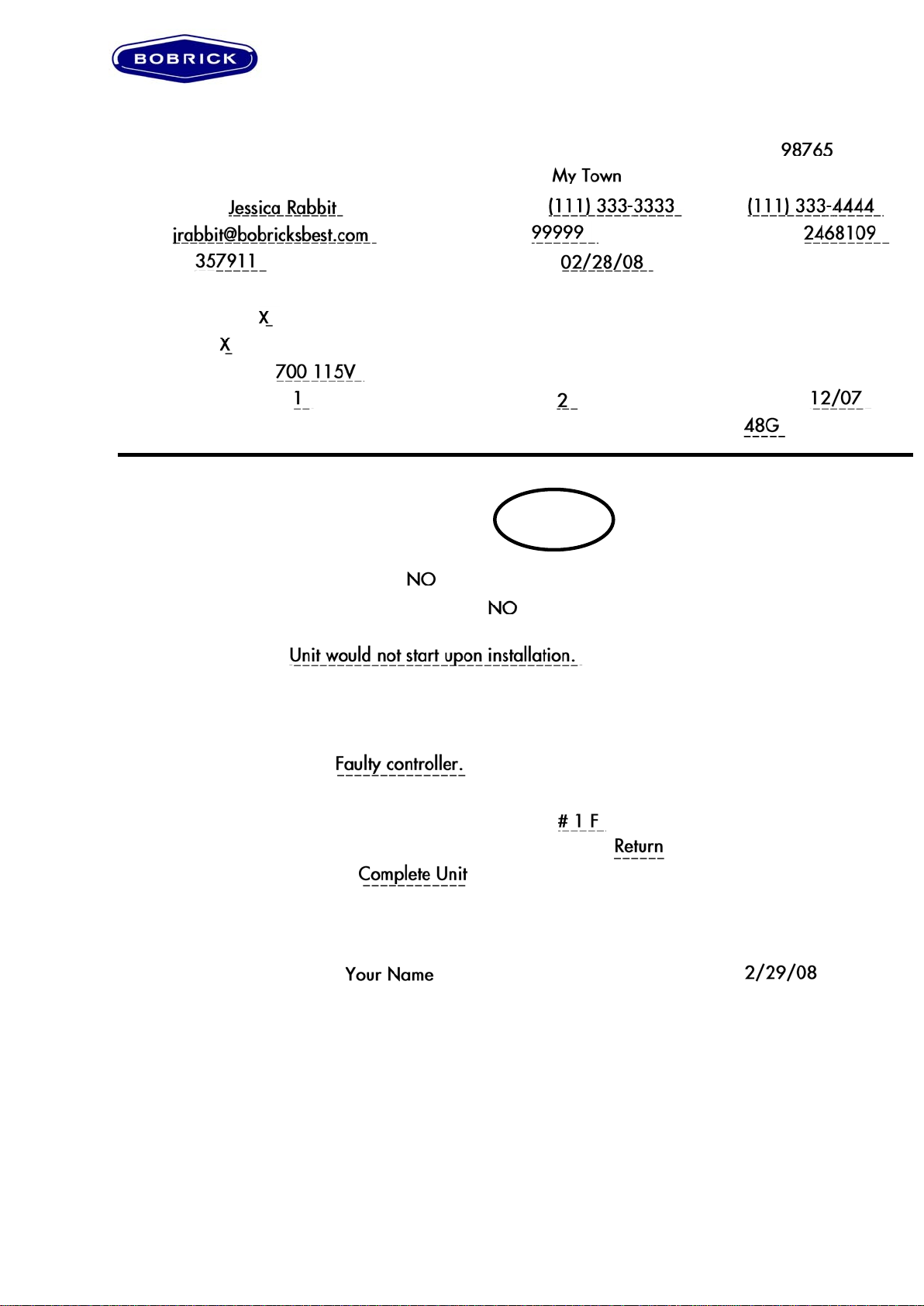
Dryer Service Information Sheet
Distributor/Rep/End-User Name: ______________________________________________________________
Address:___________________________________________________________________________________
City: _________________________________ State: ______________________ Zip code: ______________
Job Name: ____________________________ Job Location: ________________________________________
Contact name: _________________________ Telephone: __________________ Fax: __________________
Email:________________________________ Account #: __________________ Sales order #:___________
Invoice #: _____________________________ Invoice Date: ________________
Dryer Model Information:
Automatic Dryer: _______ TouchButton Dryer: _______ (check one)
Hand Dryer: _____ Hair Dryer: _____ (check one)
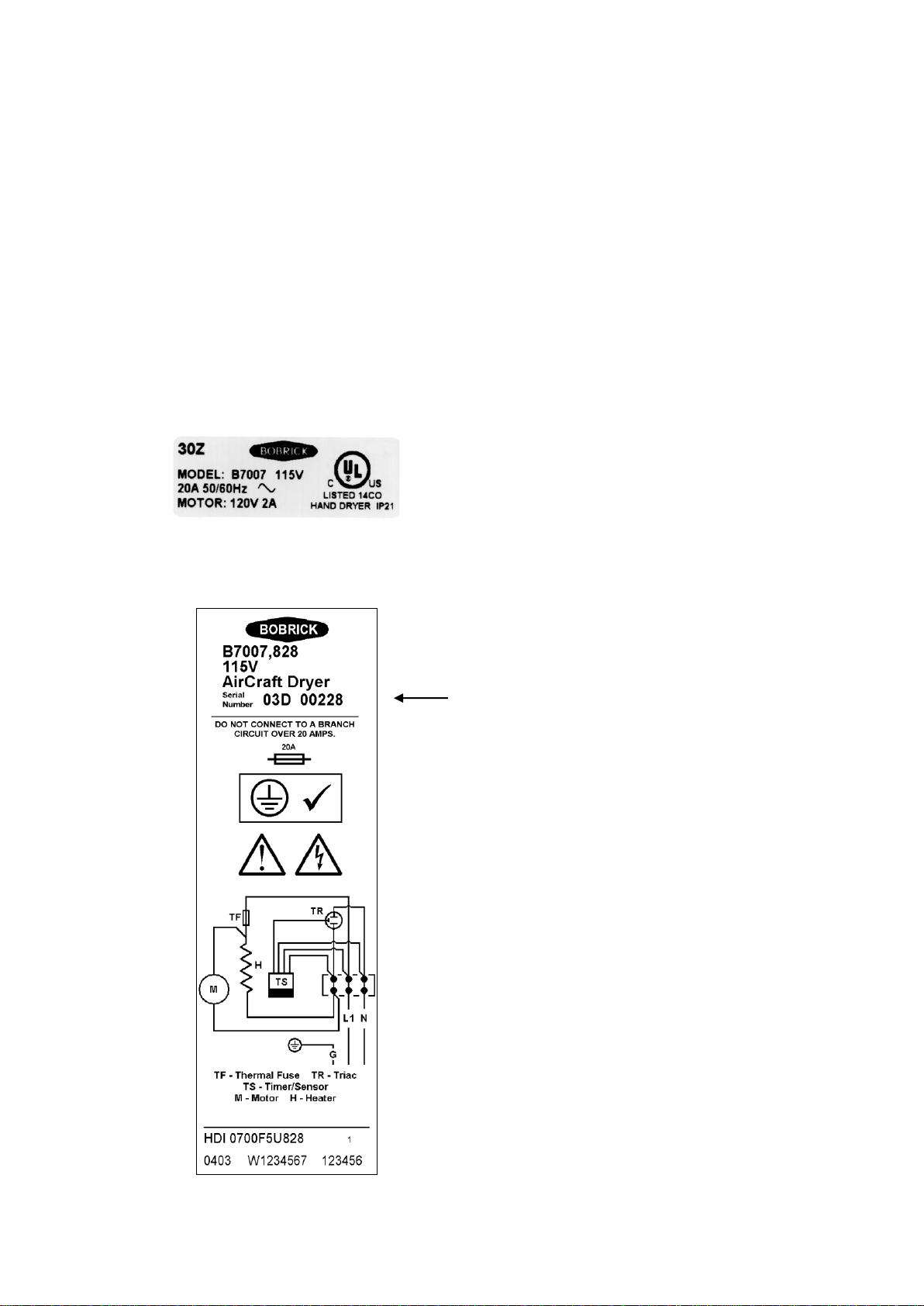
Dryer model #/voltage:___________________________________________
Quantity defective:_____________ Quantity on job: _________________ Date of installation: ___________
Date code (as seen on bottom edge of cover on dryer UL label. For example: 04A):________________________
Dryer Information:
When did dryer problems first occur from date of installation? Upon 0–2 2+ Out of
Installation Months Months Warranty
If dryer problem occurred within two months of installation, REPLACE dryer and return faulty dryer.
Does the dryer in any way function now? ______ (Yes or No)
Has the dryer been cleaned in the past 6 months? ______ (Yes or No) If No, send a cleaning sheet and
await outcome.
Full description of fault: _______________________________________________________________________
__________________________________________________________________________________________
Reference to Diagnostic Sheets:
Problem and possible solution: _________________________________________________________________
__________________________________________________________________________________________
Problem number(s) (as seen in left margin on diagnostic sheet): _______________________________________
Repair kit/parts required (if dryer needs to be returned write RETURN):__________________________________
Part number(s) for replacements: _____________________________ Replaced on SO #: ________________
ANY DEFECTIVE PARTS MUST ACCOMPANY THIS COMPLETED SHEET TO BOBRICK’S SERVICE
DEPARTMENT.
Information sheet completed by: ______________________________ Completion Date:__________________
Branch/Rep Firm: _________________________________________________________
White Copy: To Repair/Returns Department at Appropriate Branch (attached to RGA)
Yellow Copy: To BLA Customer Service for Internal Routing
Pink Copy: To Customer Service Files at Appropriate Branch
Form No. CSD-1196 ST Rev. 2/02 Bobrick Washroom Equipment, Inc. Printed in U.S.A.
12345 Your Street, Suite 100
_________________________
_____________________________
___________________________________________
Does the dryer in any way function now? ______
Has the dryer been cleaned in the past 6 months? ______
_______________________________________________________________________
_______________________________________
________________________________