14 15
Español
ADVERTENCIAS
»Una técnica de inyección o un volumen inyectado incorrectos pueden pueden causar
un rendimiento insatisfactorio y exigir una operación quirúrgica correctiva.
»Una selección incorrecta del paciente puede tener resultados desfavorables.
»Realice una toma de orina y un cultivo microbiológico para asegurarse de la
ausencia de infecciones en el tracto urinario. No proceda si el paciente tiene
infección en el tracto urinario.
»Macroplastique no se recomienda generalmente para la colocación de tejido fibrótico
o en pacientes que hayan sido anteriormente tratados con politetrafluoroetileno
o con implantes de partículas rígidas para la incontinencia, o con neoplasia maligna.
»Las inyecciones en la uretra o en el espacio suburetral exigen precisión y sólo deben
ser realizadas por cirujanos con experiencia en el diagnóstico y en la cistoscopia
terapéutica.
»No utilice catéteres internos en el posoperatorio.
»Si hay daños visuales en la jeringa o en los embalajes interior o exterior, no se
garantiza la integridad del producto y éste no debe utilizarse. Devuelva todo el
embalaje a Uroplasty o a su distribuidor para recibir otro nuevo.
»Para una inyección segura y adecuada de Macroplastique, utilice sólo las agujas
facilitadas o aprobadas por Uroplasty.
»La reutilización de un dispositivo Macroplastique abierto está asociada a riesgos de
infección y a la incapacidad para extraer el producto mediante una aguja debido a la
pérdida de humedad.
REACCIONES ADVERSAS
»Complicaciones generales asociadas con anestesia, métodos procesales y tolerancia
general del paciente al material inyectado.
»En el periodo posoperatorio pueden darse casos de disuria, hematuria y micturición
frecuente. Instruya al paciente para que se ponga en contacto con el cirujano si alguna
de estas enfermedades persiste pasadas las 48 horas.
»Puede ocurrir una retención posoperatoria que puede necesitar una cateterización
intermitente. Si el paciente sigue siendo incapaz de evacuar libremente, puede ser
necesaria una cateterización intermitente continua.
»Si el procedimiento es seguido por reacciones superiores a las esperadas, deben
establecerse procedimientos de diagnóstico y terapéuticos según la opinión del cirujano.
»Avise a Uroplasty o a su distribuidor si observa complicaciones relacionadas con
el producto acontecidas por el uso de este dispositivo.
CONSIDERACIONES TÉCNICAS
»Los cirujanos deben estar familiarizados con las características del flujo de
Macroplastique antes de la inyección.
»El volumen de Macroplastique inyectado es aproximadamente igual al volumen
permanente que ocupará cuando se forme la red de colágeno.
»Administre el producto lentamente y espere 30 segundos antes de retirar la aguja
del lugar de la inyección. Si se aplica la inyección demasiado rápido, Macroplastique
puede seguir pasando por la jeringa bajo presión.
»Inyecte Macroplastique en el tejido submucosal o en la uretra (para SUI) o en el
espacio suburetral (para VUR). Utilice una técnica adecuada de tunelización y evite
la inyección de producto demasiado superficial o demasiado profunda (ver “Técnica
de tunelización”).
»La inyección superficial causará daños en la mucosa y la pérdida de los implantes.
La implantación bajo la submucosa resultará en un bolo que puede ser demasiado
profundo para producir el material expansor del volumen del tejido deseado.
»No abra el embalaje hasta el momento inmediatamente anterior al uso. El producto
puede secarse y dificultarse así la inyección.
»Siga una técnica aséptica estricta durante la inyección.
CUIDADO PREOPERATORIO DEL PACIENTE
1. Realice una toma de orina y un cultivo microbiológico para asegurarse de la
ausencia de infecciones en el tracto urinario. Descarte una infección sistémica.
2. Administre antibióticos profilácticos de amplio espectro.
3. Pida al cliente que evacue antes del procedimiento.
4. Coloque al paciente en posición de litotomía modificada. Limpie el área con la
preparación cutánea quirúrgica y coloque vendas estériles.
5. Prepare al paciente con sedación consciente local o anestesia general.
6. Inserte 20 cc de gel de lidocaína al 2% en la uretra con la sonda de administración
del proveedor. Administre un bloque de lidocaína transuretral o periuretral. Espere
a que la anestesia local surta efecto. Nota: las inyecciones de anestesia individual
>1 ml pueden causar la hidrodisección del tejido uretral en una deposición de bolo
inestable y pueden poner en riesgo el procedimiento.
7. Llene la vejiga al 50% de su capacidad.
PROCEDIMIENTO: PREPARACIÓN DEL SISTEMA
1. Retire asépticamente la jeringa Macroplastique de su embalaje. Mantenga el
protector en la punta de la jeringa.
2. Deslice el adaptador por la jeringa del material expansor del volumen hasta que
entre en las pestañas de la jeringa. Bloquee el adaptador montado y la jeringa en el
dispositivo inyector. Sujete firmemente el adaptador y el cuello giratorio para fijar la
jeringa al dispositivo inyector. El cuello giratorio mantiene el dispositivo inyector en
una posición constante mientras rota la jeringa/aguja.
3. Retire asépticamente la aguja endoscópica de su embalaje. Sin retirar la funda
protectora de la aguja, acople la aguja endoscópica apretando firmemente el centro
de la aguja en la punta Luer lock de la jeringa. Retire la funda protectora de la aguja.
4. Antes de insertar la aguja en el cistoscopio, prepare la aguja tirando y soltando la
palanca del dispositivo inyector varias veces hasta que el producto se vea en la
punta de la aguja.
5. Pulse el mecanismo de expulsión en la parte superior del dispositivo inyector para
detener el flujo del producto.
TRATAMIENTO PARA LA INCONTINENCIA MASCULINA Y FEMENINA
Nota: al utilizar el Sistema de Implantación Macroplastique (MIS), consulte el folleto que
lo acompaña.
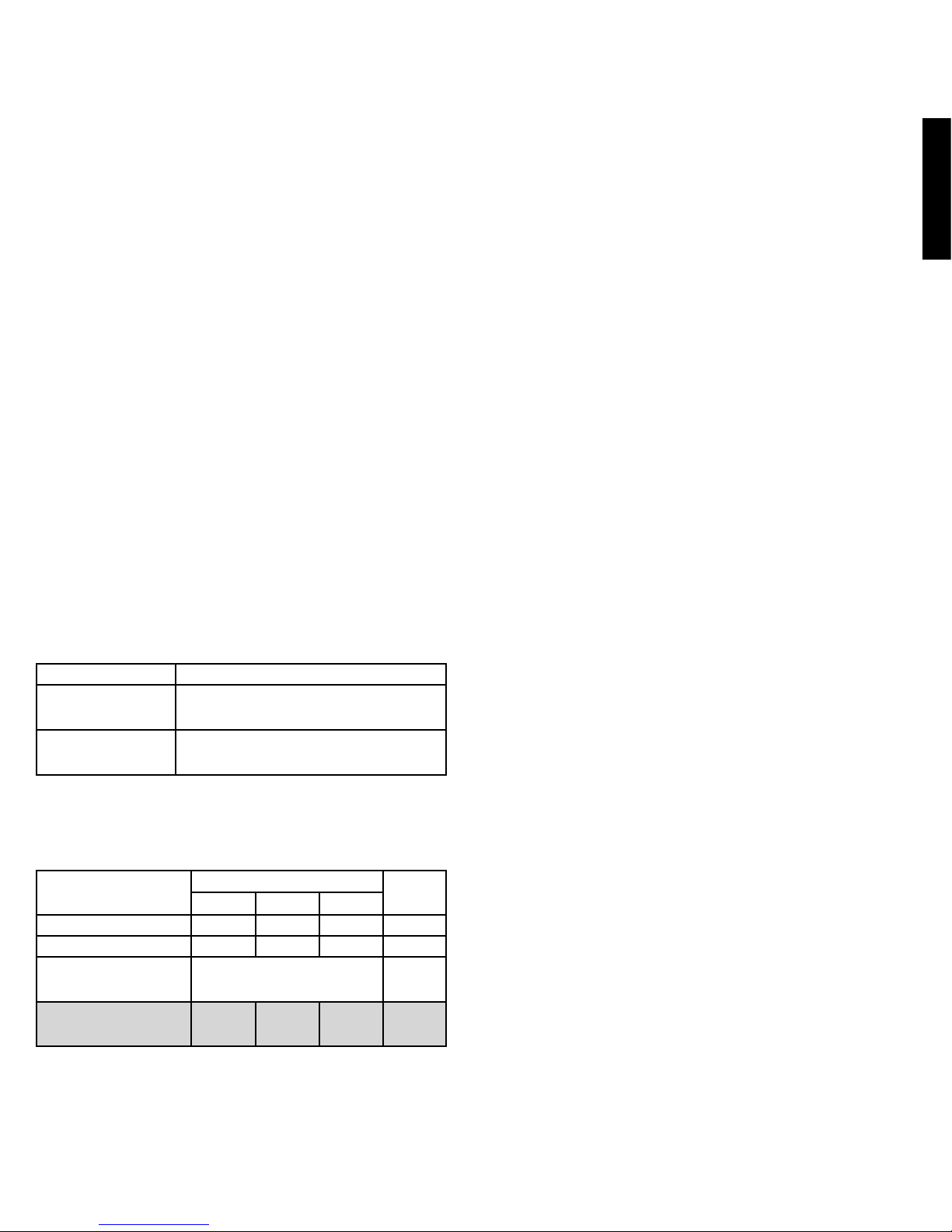
Puntos de inyección de Macroplastique
Mujeres Inyectar a 1,5 – 2,0 cm distal al cuello de la vejiga
Hombres
longitud funcional del esfínter
ext. ≤1,5 cm
Inyectar en la parte más distal del esfínter externo, pero antes
de la uretra bulbosa.
Hombres
longitud funcional del esfínter
ext. ≥1,5 cm
Inyectar a 10 mm distal al punto medio del esfínter externo. La
zona debe tener una buena vascularización y el mínimo tejido
cicatrizal.
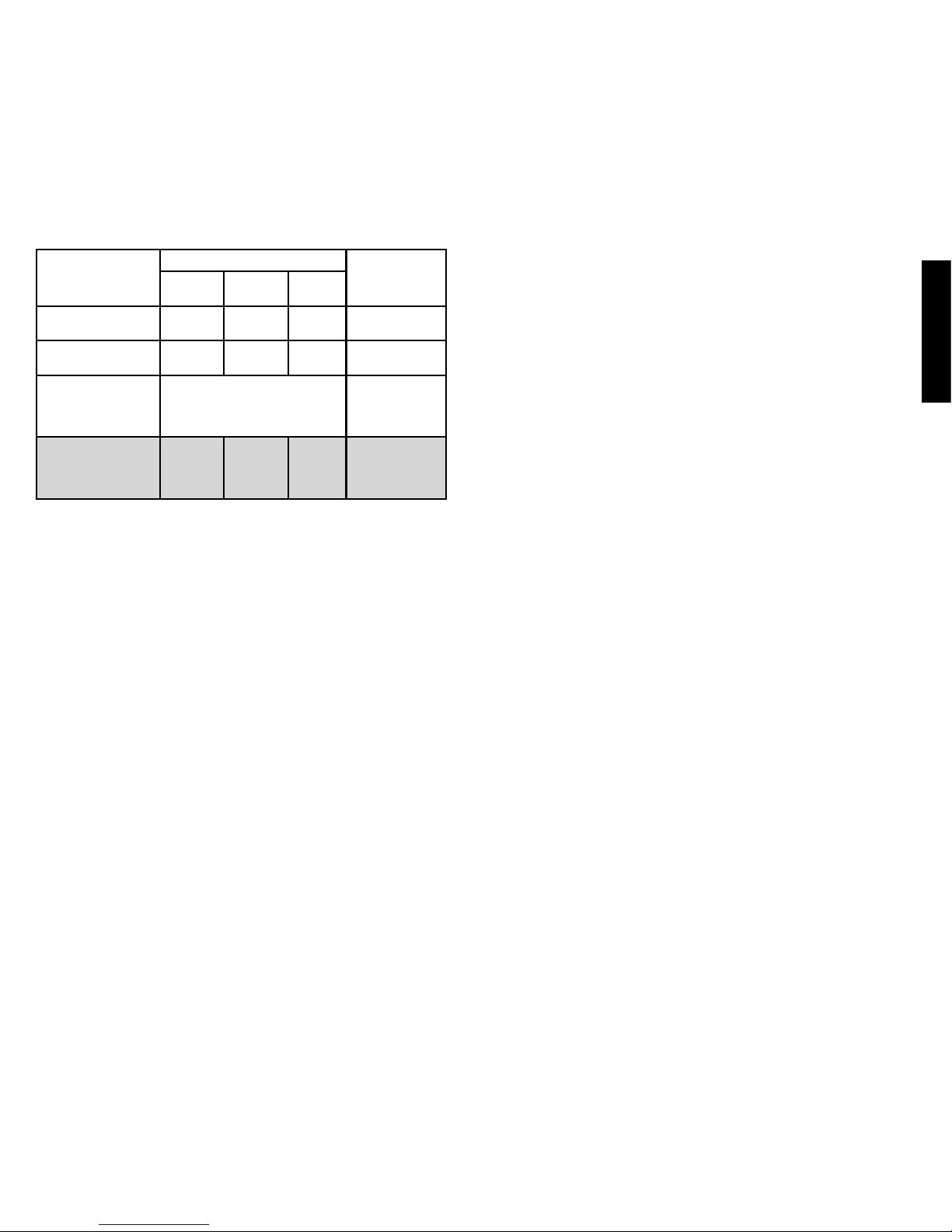
Volúmenes y posiciones aproximados para el tratamiento
Macroplastique debe ser inyectado en 2-3 posiciones alrededor de la uretra para lograr
la coaptación uretral. Las posiciones y volúmenes de inyección deben ser ajustados
de acuerdo con el historial de cirugía por incontinencia del paciente (operaciones de
suspensión del cuello de la vejiga, cabestrillo, etc.) y con la morfología del cuello de la
vejiga y de la uretra.
Posiciones aproximadas Volumen
total
6 en
punto
10 en
punto
2 en
punto
Mujeres - Tratamiento primario ≤ 2,5 ml ≤ 1,25 ml ≤ 1,25 ml ≤ 5 ml
Hombres - Tratamiento primario ≤ 2,5 ml ≤ 2,5 ml ≤ 2,5 ml ≤ 7,5 ml
Retratamiento
tras una operación anterior de
inyección de material expansor en la
uretra
El volumen y la posición dependen de
la morfología del cuello de la vejiga y
de la uretra ≤ 5 ml
Tratamiento secundario
tras una operación quirúrgica previa
(como cabestrillos)
Opinión
del
cirujano ≤ 2,5 ml ≤ 2,5 ml ≤ 5 ml