Diamedica Glostavent Helix Manual

Page 1 of 38
© Copyright Diamedica (UK) Ltd 2017
GLOSTAVENT® HELIX ANAESTHESIA SYSTEM
INSTRUCTIONS FOR USE MANUAL
For anaesthesia and ventilation in difficult circumstances
Ventilation
Back Up
Diamedica (UK) Ltd
Grange Hill Industrial Estate
Bratton Fleming
Barnstaple, Devon
EX31 4UH, United Kingdom
Tel: +44 (0)1598 710066 Fax: +44 (0)1598 710055
Email: support@diamedica.co.uk www.diamedica.co.uk
Revision A 05-05-2017 DCN-0002
ENG
0088

Page 2 of 38
© Copyright Diamedica (UK) Ltd 2017
Read this section first .
INTENDED USE.
This device is suitable for use in hospital settings and is suitable for adult and
paediatric patients.
The Glostavent® Helix facilitates the administration of inhalational anaesthesia and
respiratory support in difficult environments, humanitarian emergency situations
and low resource settings.
FOREWORD.
This manual is intended to provide guidance on the function, performance and user
maintenance of the Glostavent® Helix Anaesthesia System. The information given in
this manual is correct at the date of publication, January 2017
Separate IFU Manuals for the UPS and Oxygen Concentrator are also included and
must be reviewed for specific Safety and maintenance requirements before use.
The policy of Diamedica (UK) Ltd is to continuously improve its products. Changes
may be made to this manual without notice being given.
Users of the Glostavent® Helix Anaesthesia System must read, understand and
follow the guidance given in this manual before using the system.
THE NEED FOR PATIENT MONITORING.
WARNING.
The Glostavent® Helix Anaesthesia System delivers mixtures of gases and vapours
which could cause injury or death to the patient. The effect of anaesthesia drugs on
individual patients can vary so that “typical” machine settings for concentrations
delivered to the patient do not necessarily ensure patient safety.
Daily set up and test instructions should be successfully carried out to ensure that
the Glostavent® Series of anaesthetic machines are in operating condition. If any
parameter or test is found to deviate from the instructions the machine should not
be used and the manufacturer should be informed immediately.
The Diamedica Glostavent Helix utilizes atmospheric air within the delivered mixture
to the patient it is therefore recommended, particularly in areas at risk of
atmospheric contamination that a single use bacteria filter is used within the patient
circuit.
Medical conditions which contraindicate the use of a Glostavent® Series Anaesthesia
System and its associated applications include any medical conditions which may
contraindicate the medical procedure itself. The ultimate responsibility for patient or
procedure contraindication lies with the anaesthetist.

Page 3 of 38
© Copyright Diamedica (UK) Ltd 2017
It is essential that the patient’s respiration and cardiovascular status are frequently
checked by the anaesthetist.
The anaesthetist is ultimately responsible for patient safety and should always have
a secondary means of maintaining patient safety.
Observations of the patient must take precedence over machine settings in judging
the condition of the patient.
If ether is the only volatile agent available, it must be vaporised in a different
vaporiser. It must not be used with the mechanical ventilator due to the risk of
explosion.
Drawover anaesthesia is contraindicated for patients below 10kg, for these patients
the machine should be used in continuous flow (see section 9).
The system is only intended to be used by Qualified Anaesthetists.

Page 4 of 38
© Copyright Diamedica (UK) Ltd 2017
THE GLOSTAVENT® HELIX MANUAL
1. INTRODUCTION
2. CLEANING, GENERAL MAINTENANCE AND DISPOSAL
3. THE PRINCIPLE OF THE GLOSTAVENT® HELIX
4. THE COMPONENT PARTS OF THE GLOSTAVENT® HELIX
5. THE GLOSTAVENT® HELIX – CONTROL AND OPERATION
6. GLOSTAVENT® HELIX ALTERNATIVE POWER SOURCES
7. TEST PROCEDURE BEFORE USE
8. USE OF THE GLOSTAVENT® HELIX IN ADULTS
9. USE IN PAEDIATRIC PATIENTS
10. TROUBLE SHOOTING
11. GLOSSARY

Page 5 of 38
© Copyright Diamedica (UK) Ltd 2017
1. INTRODUCTION
In many parts of the world anaesthetics are administered in situations far removed
from those found in modern, well equipped hospitals in wealthy countries. There may,
for example, be no oxygen, electricity or technical support. In these circumstances,
the latest sophisticated anaesthetic machines with their delicate monitoring devices
are unable to function and are rapidly consigned to the graveyard of anaesthetic
equipment which litters the developing world.
Anaesthetists working in such environments need equipment which goes beyond the
standards of those required for hospitals in rich countries. Equipment is needed that
has been specifically designed to meet the additional requirements of harsh
environmental conditions and limited infrastructure and that will continue to function
in those prevailing conditions. When advice has been sought from anaesthetists
working in these areas the following properties have been most frequently requested:
The anaesthetic machine should be:
1. easy to understand and operate
2. robust and not easily damaged
3. inexpensive to purchase and economical to run
4. maintained using locally available skills
5. safe to use in the absence of expensive electronic monitoring equipment
6.
versatile, so that the same machine can be used on any size of patient, with
a variety of volatile agents, in either draw over or continuous mode, both as an
anaesthetic machine in the operating room and a ventilator in a recovery or
intensive care unit
7. able to continue operating without interruption in the absence of oxygen or
electricity.
The Glostavent® Helix anaesthetic machine has been developed to meet these
requirements and the needs of anaesthetists working in difficult environments.
This manual has been prepared to provide practical guidance for those using the
Glostavent® Helix anaesthetic machine. It should only be operated by experienced
anaesthetists who have received specific training in its use and are fully conversant
with its operation.

Page 6 of 38
© Copyright Diamedica (UK) Ltd 2017
2. CLEANING, GENERAL MAINTENANCE AND DISPOSAL
2.1 Cleaning and maintenance
The Glostavent is designed to require minimal maintenance and cleaning, however
some basic cleaning is identified below.
The anaesthesia workstation should be cleaned daily by wiping down with a damp
cloth, care should be taken to ensure that any sharps have been removed and disposed
off safely before this is done.
It is very important to check the condition of the air filter on the Glostavent at least
once every week, and more often if the environment is very humid and dusty. If the
air filter is dirty then it must be cleaned with by washing in clean water, removing as
much water as possible and replacing.
Patient safety is the primary concern of the anaesthetist and infection control is
critical to ensuring the safety of surgical procedures.
Each Glostavent Helix is supplied with a reusable breathing circuit as these items may
come in contact with the patient and can therefore potentially pass infectious agents
from one patient to another if used improperly.
The reusable breathing tubing and Y piece provided with the Glostavent Helix should
be cleaned and disinfected according to your hospital’s infection control procedures.
If no bacteria filter is used, then the entire circuit should be cleaned and disinfected
after each patient.
Any bacteria filters and other single-use items provided should be discarded after one
use since they are not designed to be reprocessed.
Halothane decomposes over time causing the release of halides, which can corrode
metal components, particularly in the presence of moisture. For this reason,
a stabilizing agent, thymol, is added to prevent decomposition. Since thymol does not
volatilize along with halothane, it can accumulate in the vaporizer, making the control
lever stiff.
If the control lever is stiff it may be the result of accumulated thymol. You can
perform the following to try to loosen the lever:
1. Remove the vaporiser from the control panel and set to zero.
2. Turn it upside down, and shake it vigorously followed by turning the lever
until it becomes loose.
3. When the lever loosens, it should be drained and rinsed with fresh agent.
4. Attach the vaporiser to the control panel and fill with fresh halothane.
If the anaesthetist has any concerns relating to cleaning or maintenance or the
function of the Glostavent they should contact the manufacturer.
The vaporiser should not require recalibration. Any Operational calibration should
only be done following consultation with manufacturer.

Page 7 of 38
© Copyright Diamedica (UK) Ltd 2017
NOTE More detailed instructions for servicing by trained technicians can be available
upon request.
2.2 Accessories and spares
All accessories used with the Glostavent® Helix must:
Be oxygen compatible,
Be biocompatible,
Comply with the general requirements of the 93/42/EEC
European Directive
A full list of available spares is available by contacting Diamedica –
2.3 Technical data enquiries
For all Technical, performance or component related enquiries please contact
Diamedica - [email protected]
2.4 Method for disposing of the device
If the product is returned to the manufacturer at the end of its life the company will
ensure disposal in line with the Waste Electrical and Electronic Equipment Directive
(WEEE) 2012/19/EU
Page 8 of 38
© Copyright Diamedica (UK) Ltd 2017
3. THE PRINCIPLE OF THE GLOSTAVENT® HELIX
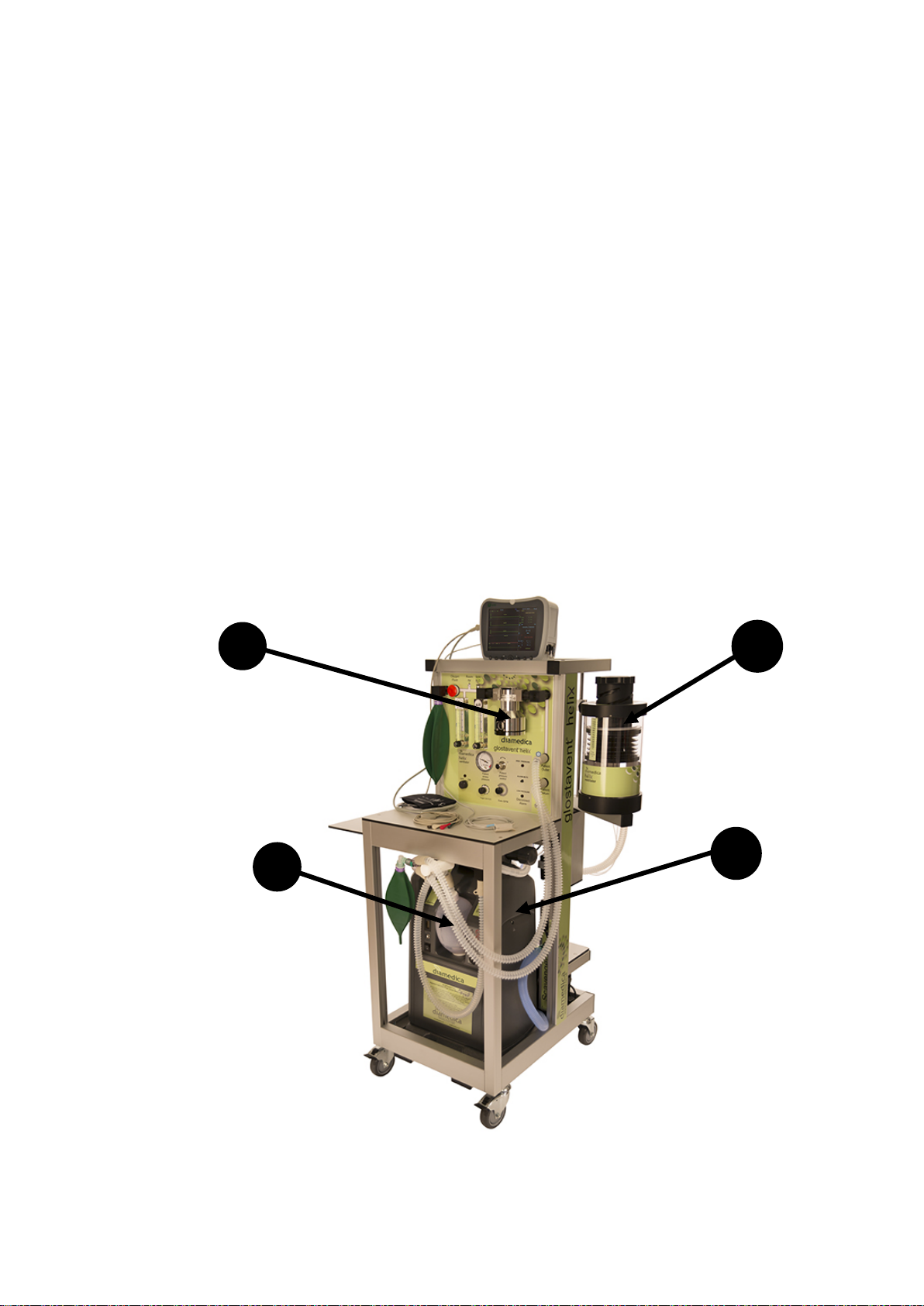
The Glostavent® Helix (Figure 1) is a free standing anaesthetic machine which has
been specifically designed to facilitate the administration of inhalational anaesthesia
in difficult environments. It is easy to understand and operate, economical to run and
can be maintained and serviced using locally available skills. Above all, it can
continue to function, without interruption, if either the oxygen or electricity supply
fails.
The Glostavent® Helix principal components which make this possible are:
1. A low resistance breathing system and vaporiser which can function in the absence
of pressurised oxygen.
2. A ventilator which is gas driven and can function in the absence of electricity.
3. An oxygen concentrator which produces oxygen and air for the patient to breathe
and oxygen to drive the ventilator.
4. An integrated method of manual assisted ventilation that can be taken to the
patient’s side.
3
2
1
Figure 1
4

Page 9 of 38
© Copyright Diamedica (UK) Ltd 2017
4. THE COMPONENT PARTS OF THE GLOSTAVENT HELIX
4.1. THE BREATHING SYSTEM.
Before a volatile anaesthetic agent can be administered to a patient it must first be
vaporised. A carrier gas containing oxygen passes through the chamber of a vaporiser
where vaporisation occurs and the resulting mixture is delivered to the patient.
Figure 2
In order for the carrier gas to pass through the vaporiser there must be a pressure
gradient between entry and exit ports of the vaporiser. The carrier gas must therefore
either be PUSHED through by positive pressure from upstream or DRAWN through
by negative pressure from downstream (Fig 2).
In the standard continuous flow type of anaesthesia machine the carrier gas is
PUSHED through the vaporiser by gases under pressure (Fig 3). Under normal
conditions, i.e. when oxygen is available, this system works well but there is one
serious disadvantage. It is entirely DEPENDENT ON AN UNINTERRUPTED
SUPPLY OF PRESSURISED OXYGEN. If the oxygen supply fails, as it frequently
does in many parts of the world, a continuous flow type of anaesthetic machine
cannot function.
Figure 3
Flow
Flow
Pressure Gradient

Page 10 of 38
© Copyright Diamedica (UK) Ltd 2017
By contrast in DRAWOVER anaesthesia the carrier gas is DRAWN over the
vaporiser by negative pressure generated by the patient’s inspiration (Fig 4). The great
advantage of draw over anaesthesia is that it can still be administered EVEN IF THE
OXYGEN SUPPLY FAILS. In this situation room air, containing 21% oxygen, can
be used as the carrier gas for the volatile agent which is supplemented with oxygen if
available.
The Glostavent® Helix can function as a continuous flow machine when gases are
provided by the concentrator or an auxiliary source. However if the electricity fails
and there is no auxiliary ‘cylinder’ oxygen available it will default to a drawover
machine in order for anaesthesia to continue safely.
Figure 4
Because of the frequency of failure of the oxygen supply in some parts of the world
the Glostavent® Helix can use either a continuous flow or a drawover breathing
system.
This conversion happens automatically in the event of gas failure or drawover can be
used in order to conserve both oxygen and anaesthetic agent. This is described further
in later sections of the manual.
The Diamedica vaporisers output is consistent in both modes, the output from other
drawover vaporisers may not suitable for both these modes.
The flow capabilities of the draw-over vaporizer are 1 – 35 L/min
PATIENT VALVE SYSTEM
Page 11 of 38
© Copyright Diamedica (UK) Ltd 2017
Features of the drawover system
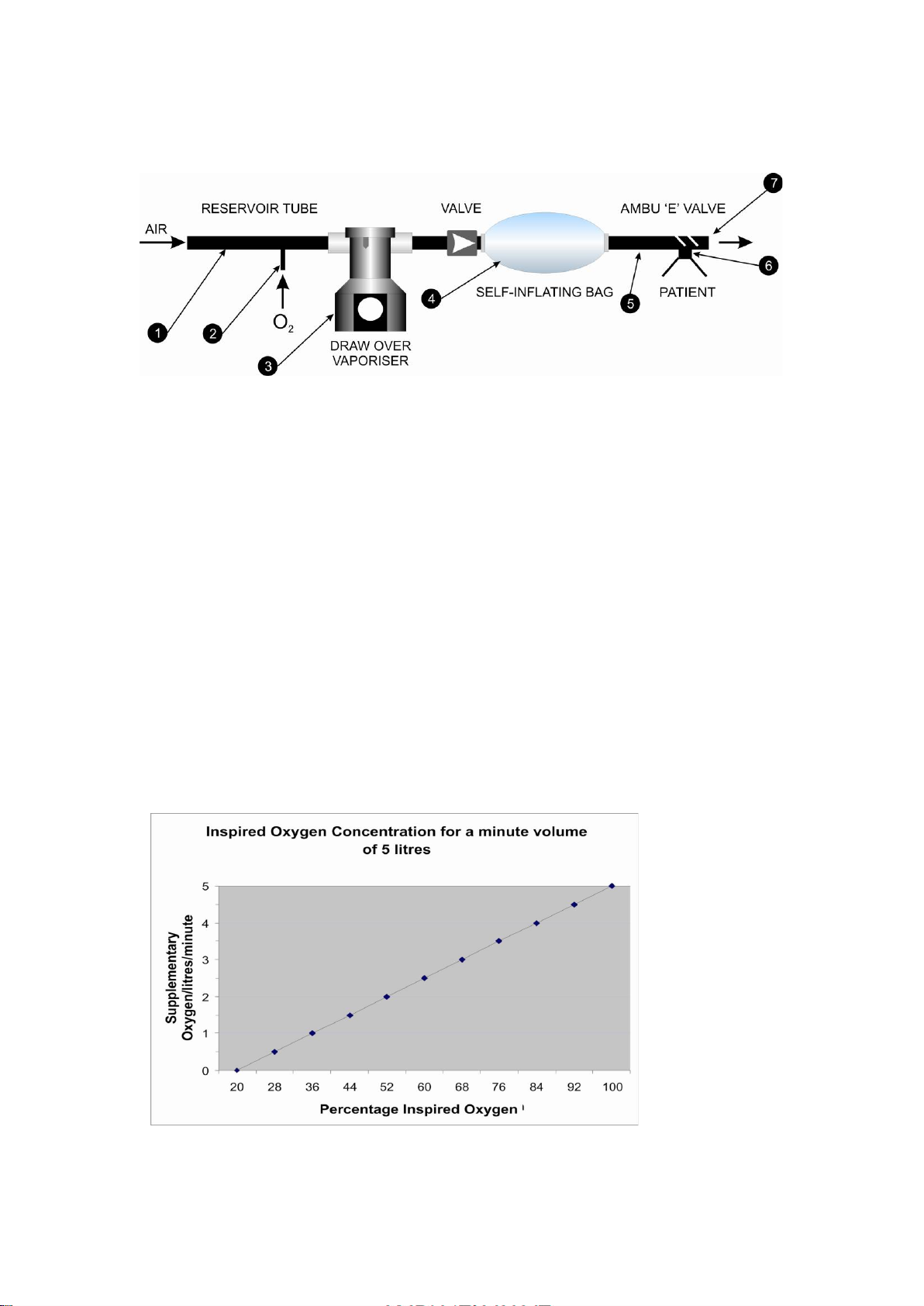
In its simplest form, a drawover system has the following features (Fig 5):
Figure 5
(1) A reservoir tube with an open end through which air is entrained during
inspiration.
(2) A side port for supplementary oxygen, if available.
(3) A vaporiser with a low resistance to breathing, such as the Diamedica vaporiser
above. (The standard plenum type vaporiser, such as the Selecta-tec, is unsuitable for
drawover anaesthesia because the resistance is too high).
(4) A self-inflating bag for I.P.P.V. with a valve to ensure the anaesthetic mixture
moves towards the patient and cannot re-enter the vaporiser.
(5) Inspiratory tubing leading to the patient.
(6) A non-rebreathing valve system that ensures that, during inspiration, the
anaesthetic mixture is not diluted by atmospheric air and that, during expiration, the
expired gas cannot re-enter the system and lead to re-breathing. The valve can
function with either spontaneous or controlled ventilation.
(7) Expiratory port leading to a scavenging system if available.
The function of the reservoir tube is to store the supplementary oxygen during the
phase of expiration so that it is not wasted and is included in the patient’s next breath.
This enables satisfactory inspired oxygen concentrations to be achieved with minimal
flows of supplementary oxygen (Fig 6).
Figure 6
In a simple drawover system the reservoir consists of a one metre length of corrugated
anaesthetic tubing. While this is satisfactory during normal breathing it is less
satisfactory during hyperventilation, for example as occurs during pre-oxygenation.

Page 12 of 38
© Copyright Diamedica (UK) Ltd 2017
This is because, when respiration is increased, more air is drawn into the reservoir and
the oxygen is diluted. To increase the efficiency of the drawover system the reservoir
has been modified for the Glostavent® by three additions (Fig 7).
Figure 7
(a) A non return valve at the open end to prevent spillage of oxygen
(b) A 2ltr reservoir bag to increase the volume of the reservoir. Movement of the
reservoir bag also provides an indication of the rate and depth of respiration.
(c) An over pressure valve set at 5 cm H2O to prevent over-distension of the reservoir
bag.
The modified reservoir conveys one other important advantage. It enables the
Glostavent® Helix to be used for both continuous flow and drawover anaesthesia
simply by adjusting the rate of gas flow in relation to the patient’s minute volume.
DRAWOVER MODE. If the patient’s minute volume leaving the reservoir exceeds
the supplementary oxygen flow entering the reservoir, the pressure in the reservoir
falls below atmospheric, air is drawn in through the open end of the reservoir tube and
the system is in drawover mode.
CONTINUOUS FLOW MODE. If the supplementary oxygen flow rate is increased
until it exceeds the patient’s minute volume, the pressure in the reservoir rises and the
system automatically transfers to continuous flow mode. In this mode any of the
standard anaesthetic breathing systems (e.g. Mapleson A, D, etc.) can be used by
substituting them for the drawover system at the common gas outlet and using the
fresh gas flow recommended for the particular system selected. A one way valve after
the vaporiser on the Glostavent® Helix prevents backflow through the system when
these circuits are in use.
Patient circuit protection
Relief valve characteristics
Circuit may contain
pressure up to 50 cmH2O
at which point the relief
valve will crack and vent
Cracking point
50cmH2O

Page 13 of 38
© Copyright Diamedica (UK) Ltd 2017
Frequently asked questions on the breathing system.
Q. What are the disadvantages of the drawover system?
A. (1) In earlier systems it was difficult to achieve high FiO2 levels during
hyperventilation such as during pre-oxygenation. This is because additional air is
sucked into the reservoir, diluting the oxygen. This problem has been largely
alleviated by the introduction of the modified reservoir.
(2) Gaseous induction requires an airtight seal at the facemask so that sub-
atmospheric pressure can be generated. This may be difficult in unco-operative
children or in the presence of facial injury. With the modified reservoir this problem
can be solved by conversion to continuous flow mode.
Q. How is the draw over system flushed with oxygen in an emergency situation?
A. There are two methods of achieving this:
a) The vaporiser is turned off and the oxygen flow meter is set to deliver the
maximum flow rate. The inspiratory limb of the circuit is briefly disconnected from
the patient while the self-inflating bag provided in the patient circuit is compressed
rapidly several times to purge the circuit of the anaesthetic mixture. It is then re-
connected and the lungs ventilated with oxygen.
b) The vaporiser is turned off and the inspiratory limb of the circuit is briefly
disconnected from the patient while the oxygen flush button on the Glostavent®
control panel is depressed for 10 seconds to purge the circuit of the anaesthetic
mixture. The inspiratory limb is then re-connected, the oxygen flowmeter is set to
maximum and the lungs ventilated with oxygen.
Q. Does the Diamedica vaporiser have any advantage over a standard plenum
type vaporiser?
A. (1) It has a low resistance allowing patients to breathe spontaneously through it.
(2) The same vaporiser can be used for a variety of volatile agents.
(3) It is less expensive.
(4) It has a simple design and can be serviced and maintained by local hospital
personnel.
Q. Which volatile agents can be used with the Diamedica vaporiser?
A. The scale is calibrated for both Halothane and Isoflurane. A Sevoflurane version
of the vaporiser is also now available. If ether is the only volatile agent available it
must be vaporised in a different vaporiser. It should not be used with the mechanical
ventilator due to the risk of explosion.
Q. How is the vaporiser filled?
A. The vaporiser is filled by unscrewing the filler cap and pouring the agent directly
from the bottle into the chamber. No special filling device is required although a
funnel is available if needed. If the vaporiser requires filling during anaesthesia then
the vaporiser must be turned off while being filled.

Page 14 of 38
© Copyright Diamedica (UK) Ltd 2017
Q. How can the vaporiser be emptied completely before a different agent is
used?
A. The door on the back of the control panel is opened and the screw supporting the
vaporiser is located so that the vaporiser can be unscrewed and removed. The filler
cap is removed and the vaporiser inverted over the bottle until fully drained using the
funnel if required. To remove the residual contents, the vaporiser is replaced, the dial
turned on fully and gas is blown through the chamber for several minutes until the
vapour can no longer be detected.
Q. How is the breathing circuit cleaned between patients?
A. The risk of contamination of the anaesthetic tubing is diminished by virtue of the
open circuit system, although bacterial filters should be used if available. The circuit
should be washed in warm soapy water between patients. For other circuits and valves
please seek the advice of the manufacturer.
Q. How can respiratory movements be monitored in drawover anaesthesia?
A. Movements of the reservoir bag can be used as a guide to the depth and rate of
respiration when using the Glostavent® Helix.
Q. What is the most effective way of pre-oxygenation of patients?
A. Satisfactory pre-oxygenation can be achieved with the Glostavent® Helix drawover
circuit using an oxygen flow rate of 10 l/min.
Q. What regular maintenance is required for the Diamedica vaporiser?
A. The vaporiser has been designed to require minimal maintenance. If movements
of the dial lever become stiff, the shuttle casing should be cleaned. A small quantity
of Halothane is poured into the chamber which is inverted and shaken several times
before being discarded.
Page 15 of 38
© Copyright Diamedica (UK) Ltd 2017
4.2. THE OXYGEN CONCENTRATOR
Cylinders of oxygen are expensive and may run out whereas atmospheric air costs
nothing and does not run out. For this reason atmospheric air is used as the principal
source of oxygen for the Glostavent® Helix delivered by means of an oxygen
concentrator. (Figure 8)
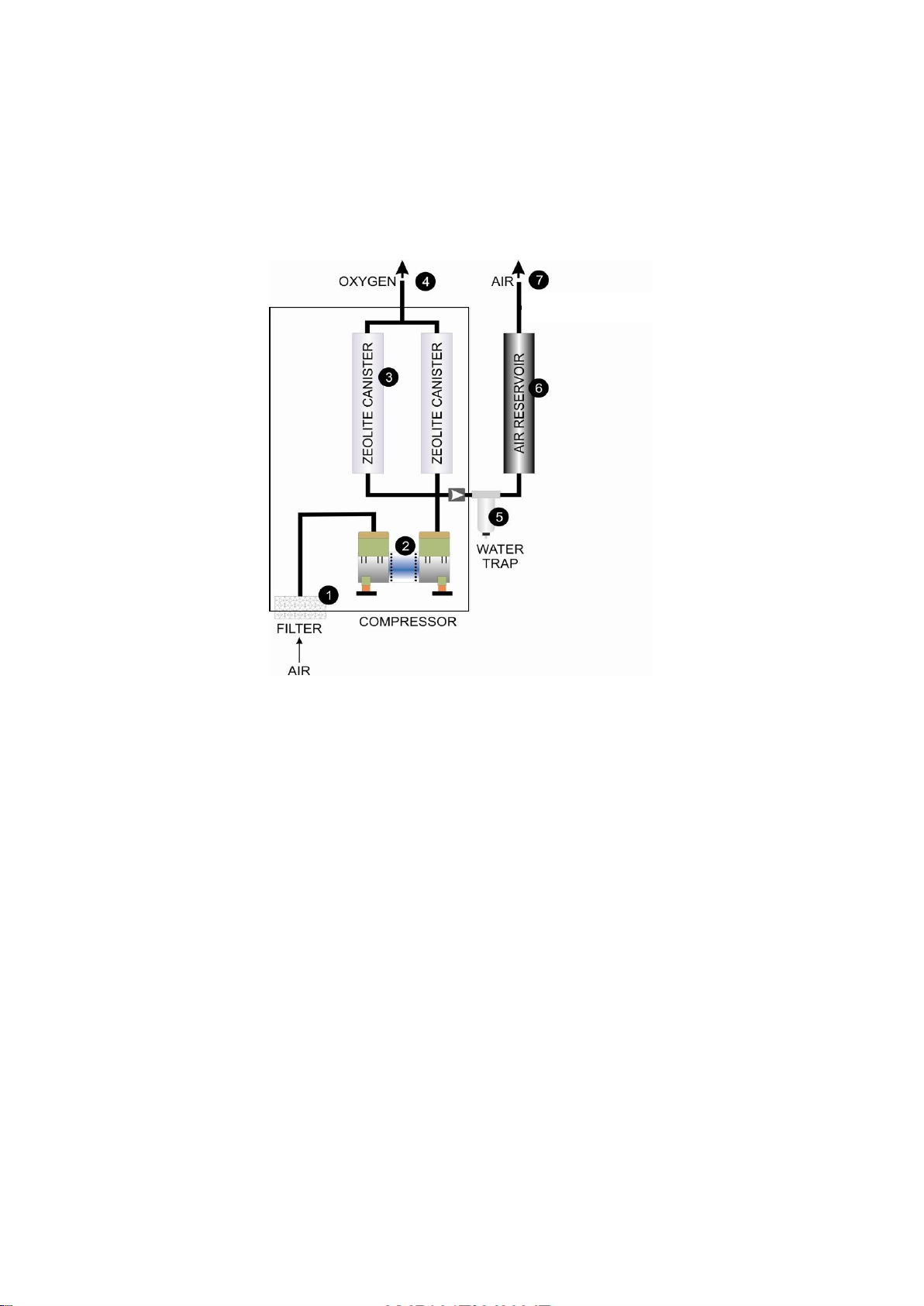
Figure 8
The oxygen concentrator is a device that can produce a supply of oxygen from
atmospheric air. The air is drawn into the concentrator through a filter (1) and then
compressed (2) to a pressure of 20 psi (140 KPa ). Some of this compressed air then
passes through canisters containing granules of zeolite (3) where the nitrogen is
absorbed and the residual oxygen delivered to the patient or used to drive the
ventilator (4). The remainder of the compressed air passes through a water trap (5)
which enables the water formed by condensation to be automatically released at
regular intervals so that it cannot obstruct the flow. It then enters the compressed air
reservoir (6) from which it is available for the breathing circuit (7).
The concentrator is able to deliver simultaneously up to 10 litres/min of oxygen and
10 litres/min of air for the patient and some of the oxygen is also used to drive the
ventilator before recycling this drive oxygen into the patient circuit. The electricity
consumption is only 590 Watts (equivalent to four electric light bulbs) and is the same
regardless of the flow of gases.

Page 16 of 38
© Copyright Diamedica (UK) Ltd 2017
Frequently asked questions on the oxygen concentrator.
Q. How often does the zeolite need changing?
A. Unlike soda lime, zeolite does not need changing as the granules are constantly
being re-charged. The same canisters can be used for many years.
Q. Can the concentrator function at high altitude?
A. Yes. It functions in the same way whatever the altitude.
Q. Can the concentrator function when the humidity is high?
A. Yes. There is a water trap in the compressed air tubing to prevent condensation
causing obstruction of the tubes.
Q. Can the concentrator function in the presence of high voltage fluctuations?
A. The UPS system incorporates a voltage stabiliser which enables the Glostavent® to
function in the presence of fluctuations of +/- 30 %.
Q. Is there any advantage in using the concentrator if cylinders are available?
A. Yes. Cylinders of oxygen are expensive and may run out. In contrast atmospheric
air costs nothing and does not run out. Therefore whenever possible air should be the
source of oxygen via the concentrator and cylinders of oxygen kept in reserve.
Q. What is the comparative cost of using oxygen cylinders as opposed to the
oxygen concentrator?
A. The cost of running the concentrator is approximately 1% of the cost of cylinder
oxygen.
Q. What are the servicing requirements of the concentrator?
A. The concentrator has been designed to require minimal servicing. The only
regular maintenance required is the cleaning of the gross particle filter located at the
air entry site at the rear of the concentrator, by washing it in warm soapy water and
leaving it to dry. This should normally be carried out every 3-4 days but more
frequently in dusty conditions.

Page 17 of 38
© Copyright Diamedica (UK) Ltd 2017
4.3. THE GLOSTAVENT ® HELIX VENTILATOR (Figure 9)
Figure 9
The tidal volume range on the Glostavent Helix is 35ml to 1200ml, the displaced
volume over this range is accurate to +/- 10% over the full range of possible BPM (4-
40)
Diamedica
Helix
Ventilator
Patient
Outlet
Patient
Return
O
2
Air
OFF ON
Patient
Pressure
Trigger BPM
High Pressure
Low Pressure
Alarm Mute
This is a time cycled, volume limited pressure
generator. It is a gas driven ventilator and can therefore
function largely independently of the supply of
electricity. There is however a small battery which is
required to power the electronic circuitry. This battery
should be kept fully charged by keeping the ventilator
connected to the mains supply when available.
The ventilator bellows section consists of a set of
bellows and a helix screw above the bellows for tidal
volume adjustment.
A drive piston is mounted below the bellows and is
driven upwards by the driving gas. This piston pushes the
top of the bellows upwards causing the bellows to
expand and fill with the gas mixture. When the control
solenoid switches the gas flow the piston is driven closed
compressing the bellows; a valve directs the gas mixture
towards the patient.
Tidal Volume
Lock
Ventilation
Back Up

Page 18 of 38
© Copyright Diamedica (UK) Ltd 2017
5. THE GLOSTAVENT HELIX - CONTROL AND OPERATION
INTER-RELATION OF COMPONENT PARTS (Fig 10)
Below the ventilator is the oxygen concentrator (1) which provides both oxygen (2) to
supplement the inspired mixture and to drive the ventilator. It also provides air (3) to
add gas flow for continuous flow operation if required.
An oxygen cylinder (4) should be available as a reserve to act as a source of oxygen
(5) for the patient (6) and to drive the ventilator in the event of failure of the
concentrator. The piston requires a driving pressure of 20 PSI (140 KPa) and can
therefore utilise either oxygen from the concentrator or oxygen from the cylinder.
Under normal conditions, i.e. when electricity is available, the concentrator supplies
both the oxygen for the patient to breathe and to drive the ventilator.
Figure 10
If the electricity supply fails, the concentrator is no longer able to function. The
reserve oxygen cylinder then takes over as the source of both the oxygen for the
patient and to drive the ventilator. This change-over occurs when valves (7) and (8)
open automatically. No intervention is required by the anaesthetist.
When the reserve oxygen cylinder is in use, conservation of oxygen assumes great
importance. This is achieved in two ways;
(1) Recycling of oxygen. After the oxygen has been used to drive the ventilator it is
collected and returned to the breathing circuit via the supplementary oxygen tube (9).
In other words, the same oxygen is used twice, first to drive the ventilator and then to
supplement the inspired gas mixture. In this way the resulting oxygen concentration
delivered to the patient is elevated to 35% without the need for any other
supplementation.
(2) The ventilator has been designed to minimise the volume of driving gas required.
This is possible because the piston diameter is much smaller than that of the bellows.
9
11
To Patient

Page 19 of 38
© Copyright Diamedica (UK) Ltd 2017
The volume of driving gas required is therefore only 1/6th of the tidal volume set for
the patient. In the unlikely event of a simultaneous failure of both oxygen and
electricity the anaesthetic can still continue safely using atmospheric air as the carrier
gas. However, because of the respiratory depressive effects of the anaesthetic agents,
controlled ventilation is required to prevent hypoxia. This can be achieved by utilising
the self-inflating bag (11) supplied as part of the breathing circuit.
Frequently asked questions on the ventilator
Q. How long can the ventilator function in the complete absence of electricity?
A. Providing oxygen is available the limiting factor is the life of the battery needed
for the electronic circuitry. A fully charged battery will last for 100 hours. It is
therefore important to keep the battery fully charged when the Glostavent® Helix is
not in use.
Q. Does the compression caused by the bellows cause distension of the self-
inflating bag and thus a decrease in tidal volume?
A. No. The self inflating bag is sufficiently rigid to resist significant expansion
during inflation of the lungs.
Q. How does the Glostavent® Helix ventilator differ from other similar
ventilators?
A. (1) The tidal volume control is absolute, so the tidal volume can be determined
accurately by the setting. This is not possible with some other similar ventilators.
(2) The bellows is suitable for adult and paediatric patients.
(3) The Helix control on the top of the bellow gives accurate volume control.
(4) There is a triggering facility to assist weaning.
Q. Can positive end expiratory pressure (PEEP) be used?
A. Yes, by applying an adjustable PEEP valve to the expiratory limb of the circuit.
Q. How much does it cost to drive the ventilator for 24 hours?
A. When the ventilator is being powered by oxygen from the concentrator, the cost
of driving the ventilator is the cost of electricity for the concentrator. In the UK this is
approximately £0.05 per hour or £1.20 per day. Oxygen supplementation can also be
provided by the concentrator at no extra cost. This would compare to a conventional
gas driven ventilator running cost of approximately £80.00 per day when running
from oxygen cylinders.
Q. Is humidification of the inspired gas required?
A. It is preferable but not essential for short term ventilation e.g. the duration of
surgery. For long term ventilation as in an intensive care unit humidification is
advisable using either a filter or humidifier at the patient’s airway.
The individual components of the Glostavent® Helix are interconnected on a mobile
workstation with a flow meter control panel above a shelf and has an arm supporting
the ventilator, and an oxygen concentrator below.
Page 20 of 38
© Copyright Diamedica (UK) Ltd 2017
Figure 11
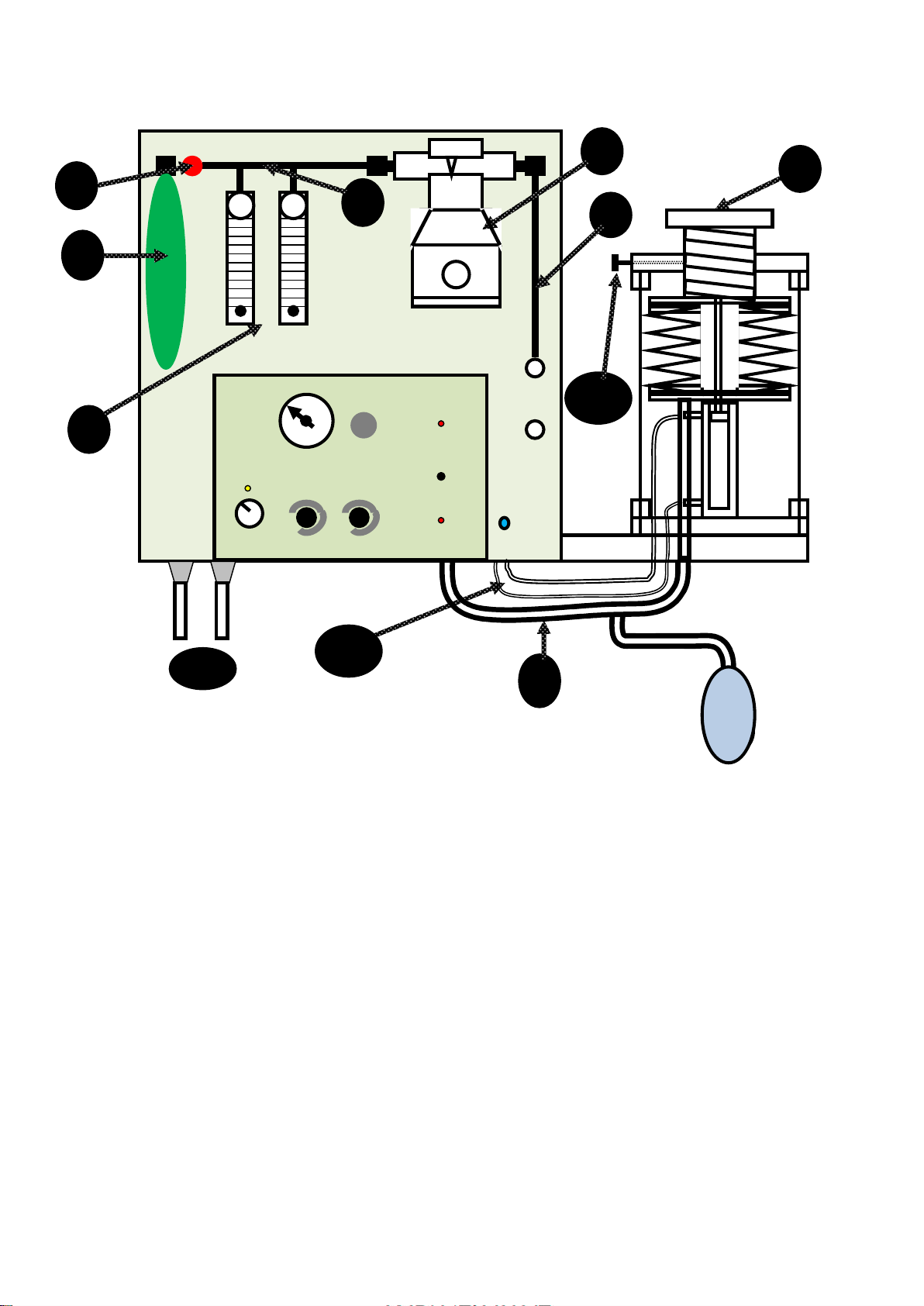
THE FLOW METER CONTROL PANEL Fig 11
Diagram on panel indicating gas pathway (1). Reservoir bag on left of panel (2). The
function of this is to increase the volume of the reservoir and provide an indication of
the rate and depth of respiration. It is not used to control or assist respiration. Bank of
flow meters (3) left: oxygen from concentrator or backup (10l/min maximum) right:
air from concentrator (10l/min maximum). Vaporiser (4) with concentration scale,
filling port and glass window. (5) Indicates the position of the tube connecting the
vaporiser to patient outlet on the panel. Note that this tube is behind the panel and
therefore not visible. It contains a one way valve to prevent back flow of the
anaesthetic gases.
A corrugated tube connects the patient outlet on the panel to the ventilator (6).
Oxygen flush button (7). To flush the patient circuit, first switch off the vaporiser, then
disconnect circuit close to the patient and depress the flush button for 10 seconds.
This will flush with oxygen at a rate of 30 l per minute. Self-inflating bag (8) for
manual/assisted ventilation. Helix screw (9) for tidal volume adjustment. Ventilator drive
gas and return (10). Oxygen and Air connections from the oxygen concentrator (11). Tidal
volume lock (12).
5
6
4
3
2
1
7
8
9
10
0 1 2 3 4 5
11
Diamedica
Helix
Ventilator
Patient
Outlet
Patient
Return
O
2
Air
OFF ON
Patient
Pressure
Trigger BPM
12
Ventilation
Back-up
High Pressure
Alarm Mute
Low Pressure
Other manuals for Glostavent Helix
1
Table of contents
Other Diamedica Medical Equipment manuals
























